
[ad_1]
In a recent study published in the journal Scientific Reports, researchers used self-reports and wearable sensors to investigate the relationship between body temperature and depression, examining minor variations between awake and sleeping body temperature and reduced diurnal body temperature amplitude.
Depression is an important health issue in the United States, with significant expenses for teenagers and young adults. Antidepressant usage has expanded in Western countries, yet existing pharmacologic medicines have limited effectiveness. It is critical to understand the processes that cause depression symptoms and recognize modifiable ones to create innovative therapies. Identifying anomalies related to depression may lead to a biologically homogenous subgroup that responds better to therapies targeting particular abnormalities.
 Study: Elevated body temperature is associated with depressive symptoms: results from the TemPredict Study. Image Credit: DimaBerlin / Shutterstock
Study: Elevated body temperature is associated with depressive symptoms: results from the TemPredict Study. Image Credit: DimaBerlin / Shutterstock
About the study
In the present study, researchers explored the association between body temperature and depression using data from the TemPredict Study, which included over 20,000 individuals in seven months. Eligible participants were adults who could converse in English and had mobiles that could link with the wearable sensor.
The researchers investigated whether higher self-measured body temperature, lower daytime distal-region body temperature amplitudes, and minor differences between awake-time and asleep-time distal temperatures were associated with increased severity of depression. The team collected data on self-measured body temperatures, wearable sensor-recorded minute-level distal-region body temperatures, and self-reported depressive symptoms. The participants measured body temperature once a day with standard thermometers, and wearable sensors measured minute-level distal temperatures recorded using negative temperature coefficient (NTC) thermistors.
The team sent the participants monthly surveys via email containing the Patient Reported Outcomes Medical Information System (PROMIS) Profile instrument for depressive symptoms experienced in the previous month. They converted the raw PROMIS depression summary scores into T-scores. In baseline surveys, participants self-reported demographic information such as age and sex.
The researchers used linear regression models to construct odds ratios (ORs) to investigate the association between the mean daily self-documented body temperatures and the PROMIS T-scores. They calculated E-values for sensitivity analyses. The team computed the difference between the daily maximal and minimal distal body temperatures for all individuals to determine the amplitudes for daytime distal body temperatures.
Results
The mean age of the research participants who self-reported their body temperature was 47 years, with 53% being male. Participating individuals completed 3.60 of the seven available PROMIS depression tests. The sensor-recorded body temperatures sample consisted of 21,064 participants, with a mean age of 47 years and 56% men. In both unadjusted and adjusted models, the researchers discovered a positive connection between body temperature and depression T-scores. Linear models had E-values higher than the effects of age, sex, and body temperature on depression.
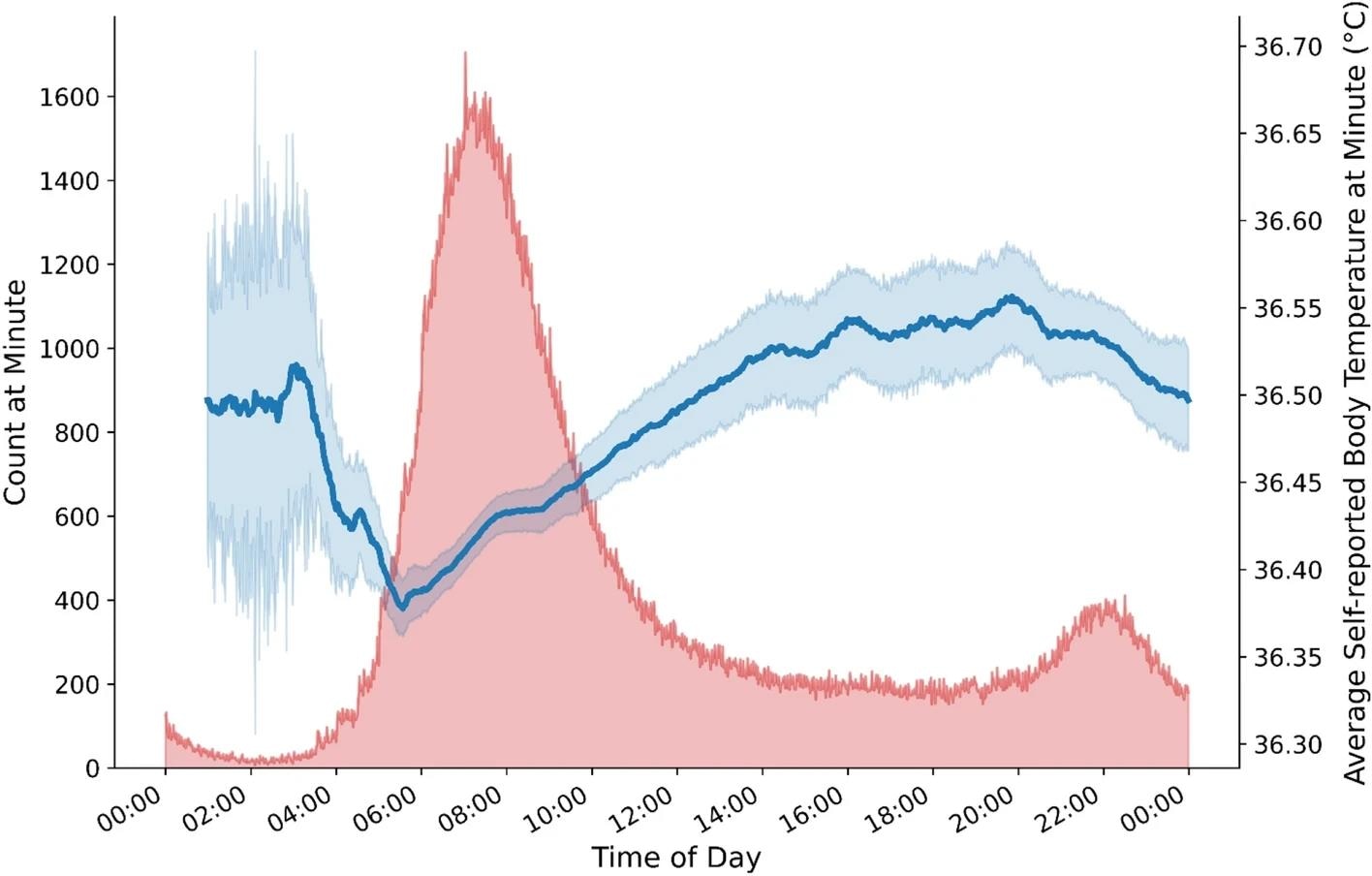 Average self-reported body temperature by time-of-day. Figure depicts expected diurnal pattern of lowest self-reported body temperatures reported in the early morning hours and higher self-reported body temperatures during daytime hours. Note. Blue line depicts average self-reported body temperature (right Y axis) by time of day; blue shading indicates standard error of the mean. Red shading indicates number of responses (left Y axis) provided at each minute (X axis).
Average self-reported body temperature by time-of-day. Figure depicts expected diurnal pattern of lowest self-reported body temperatures reported in the early morning hours and higher self-reported body temperatures during daytime hours. Note. Blue line depicts average self-reported body temperature (right Y axis) by time of day; blue shading indicates standard error of the mean. Red shading indicates number of responses (left Y axis) provided at each minute (X axis).
The adjusted regressions revealed that body temperatures accounted for unique variances in PROMIS T-scores, while known variances were accounted for by age and gender. The OR value for having mean PROMIS T-scores in the moderate versus normal range increased significantly with every 0.10°C rise in the mean body temperature (OR, 1.0). PROMIS T-scores in moderate and severe ranges (OR, 1.1) were more likely present than within the normal range.
The team used the receiver-operating characteristic (ROC) curves to analyze PROMIS T-scores, revealing improved differentiation between severe, moderate, and mild depression severity levels, with ROC curve values of 0.8, 0.7, and 0.6, respectively. Based on the corrected model, Youden’s Index has 86% sensitivity in detecting PROMIS T-scores for depression in the severe range but only 34% specificity. The unadjusted model performed best, with 97% sensitivity to identify PROMIS T-scores in the moderate range (with 63% specificity).
The awake-time distal body temperatures changed slightly higher from the normal range to mild to moderate, with the most marked shift occurring from WNL to severe depression symptoms. Associated statistical tests revealed significant differences in awake-time distal body temperatures, asleep-awake differences in the distal body temperatures, and amplitudes for daytime distal body temperatures, comparing these metrics among participants with severe symptoms and within the normal range. Individuals with severe depression symptoms showed the highest difference in distal body temperatures compared to those with depression symptoms within the normal range.
Overall, the study findings showed depressive symptoms associated with higher awake-time body temperatures. The collection of thermometer-measured and wearable sensor-recorded body temperatures corroborated the association. Asleep-time distal temperatures were comparable across the different categories of depression and greater than awake-time distal body temperatures, resulting in decreased asleep-awake disparities as depressed symptom severity increased. Individuals who directly target thermoregulatory systems have reported antidepressant effects.
Journal reference:
- Mason, A.E., Kasl, P., Soltani, S., et al. Elevated body temperature is associated with depressive symptoms: results from the TemPredict Study. Sci Rep 14, 1884 (2024), DOI: 10.1038/s41598-024-51567-w, https://www.nature.com/articles/s41598-024-51567-w
[ad_2]
Source link
