[ad_1]
Nature, Published online: 06 November 2024; doi:10.1038/d41586-024-03636-3
Mitochondria form two distinct subpopulations enabling them to produce essential cell components and energy, even under nutrient stress.
[ad_2]
Source link

[ad_1]
Nature, Published online: 06 November 2024; doi:10.1038/d41586-024-03636-3
Mitochondria form two distinct subpopulations enabling them to produce essential cell components and energy, even under nutrient stress.
[ad_2]
Source link

[ad_1]

Many women live with endometriosis but scientists say research into the condition is underfunded.Credit: GARO/PHANIE/Science Photo Library
Pain-sensing nerves and immune cells work together to wreak havoc in endometriosis, a painful condition that affects an estimated 190 million women and girls of reproductive age. But a study in mice suggests a way to harness that interaction to treat the disorder1.
The research, which was published on 6 November in Science Translational Medicine, reveals a key molecular pathway that not only promotes the sensation of pain caused by endometriosis, but also exacerbates the disease. Drugs that inhibit this pathway are already used for the treatment of migraines — the study’s findings suggest that these therapies might be useful to treat endometriosis as well.
“This is a new way of looking at how we could change pain pathways in endometriosis,” says Louise Hull, a researcher who studies endometriosis and treats people with the condition at the University of Adelaide in Australia.
Endometriosis occurs when cells similar to the lining of the uterus grow outside of the organ, sometimes causing pain, infertility and heavy menstrual bleeding. Current treatment options are limited. Hormonal medications can reduce symptoms in some people but not everyone can tolerate the side effects, and they are not useful for those who want to become pregnant. Non-steroidal anti-inflammatory drugs are used to relieve pain, but long-term use can damage the liver and kidneys. And the benefits of surgical treatments to remove endometrial deposits are often transient.
The condition is also famously understudied, says Michael Rogers, a cancer researcher at the Boston Children’s Hospital in Massachusetts and an author on the study. “Compared to other diseases that are similarly widespread and have a similar economic impact, endometriosis research is at least two — and probably three — orders of magnitude underfunded,” he says.
Rogers was recruited to the field by a member of his church whose family has been severely affected by endometriosis. Every month or two, she petitioned him: “She would say, ‘Mike, you really need to start working on this disease.’”
Eventually, she won him over. Rogers started following research in the field and, about nine years ago, began to develop the animal models he needed to investigate the condition.
By then, researchers had already discovered that immune cells called macrophages probably contribute to endometriosis and that pain-sensing nerves are also involved2. Rogers and his colleagues found that disabling these nerves in mice with a condition similar to endometriosis not only dampened pain, as assesed by the animals’ behaviour, but also reduced the size of lesions containing endometrial cells. “This strongly suggested that the pain-sensing nerves weren’t just sensing pain, they were doing something to help the lesions grow,” says study co-author Victor Fattori, a pharmacologist at Boston Children’s Hospital.
The team decided to test whether a protein called CGRP, which aids communication between the nervous system and macrophages, might also have a role in endometriosis. Several drugs that block CGRP have already been approved by the US Food and Drug Administration for other conditions, and the researchers administered four of these to mice that model endometriosis.
Again, they saw a decrease in pain. Two of the drugs significantly reduced lesion size, and it’s possible that higher doses of the other two medicines would have as well, says Rogers.
Clinical trials are needed to determine whether the same approach could be effective in people. Rogers is optimistic that such trials could begin soon: the drugs are already on the market and are considered relatively safe.
Even so, it will be particularly important to demonstrate that they are safe for women who might want to become pregnant while taking the drug, says Hull.
If shown to be safe and effective, CGRP-inhibiting drugs could fill a gap in care for people with endometriosis, says Erin Greaves, who studies the condition at the University of Warwick, UK, and who collaborates with Rogers. “New non-hormonal treatments for endometriosis are desperately needed.”
[ad_2]
Source link

[ad_1]

Mapping tumours and the genetic changes within them could help develop new cancer treatments
Sipa Press/Alamy
We now have some of the most detailed maps ever made of several cancers, along with new tools and methods for analysing them. The findings come from an initiative to map cancers called the Human Tumor Atlas Network, and provide clues about how cancers form, evolve and become resistant to treatment.
Cancer develops when genetic mutations spur cells to grow and proliferate uncontrollably. Much of what we know about the disease comes from genetically analysing tumours. Until recently, we could only do this by combining and analysing all the genetic data in a tumour sample at once, making it impossible to identify individual cell types.
But tumours aren’t monolithic. “They’re complex, like ecosystems that consist of not just tumour cells, but also immune cells, endothelial cells and other support cells,” says Daniel Abravanel at the Dana-Farber Cancer Institute in Boston.
Thanks to the advent of more sophisticated tools, a team of researchers has now been able to identify individual cells or determine their functions in tumours from nearly 2000 people with 20 different kinds of cancer.
As part of the work, Li Ding at Washington University in St. Louis, Missouri, and her colleagues mapped 131 tumour regions from 78 people with cancer types that show up in the breasts, colon, pancreas, kidneys, uterus and the bile ducts that connect the liver and gall bladder to the small intestine. They used a technique called single-cell sequencing to measure which genes were turned on or off in each cell of a tumour sample.
The researchers also viewed tissue samples under powerful microscopes to determine the location and structure of cells. Next, they built 3D models of tumours, showing how cells within them are organised and interact. They found that, within tumours, cancer cells form distinct clusters known as microregions. The researchers then grouped these areas based on similar genetic alterations, such as high or low immune cell activity. Evolution within the genetic activity of cells in microregions appears to be a major factor in cancers becoming resistant to treatments.
Further research from the Human Tumor Atlas Network suggests that multiple cells can sometimes coordinate to form colon cancer. “For decades, the consensus in the field has been that a tumour originates from a single cell,” says Doug Winton at the University of Cambridge.
Winton and his colleagues used mice that were genetically engineered so their cells changed colour when they became cancerous. This made it possible to identify and track tumours as they formed in the guts of the animals. The researchers found that about 40 per cent of colon tumours originated from multiple cells, which cooperated to outcompete neighbouring cells.
A separate group of researchers led by Ken Lau at Vanderbilt University in Tennessee also identified biomarkers for monitoring tumour evolution. Naturally occurring mutations create permanent genetic changes in tissue, which allowed the researchers to reconstruct the sequence of events, creating a molecular timeline of each tumour’s growth.
Using this approach, they analysed early precursors of colon cancer in mice and people and found that up to 30 per cent had a multicellular origin. The best predictor we currently have for determining whether a precancerous lesion in the colon will become cancerous is its size, says Lau. Understanding how colon cancer forms can improve our ability to screen precancerous lesions and detect cancer earlier, he says.
The cancer mapping project uncovered some surprises. Abravanel and his colleagues collected 67 tumour biopsies from 60 people with metastatic breast cancer, meaning it had spread to other organs, such as the liver, brain and lungs. They found that samples collected from the same participant at different time points were genetically very similar. “You would expect to see different mutations evolve over time,” says Abravanel.
As part of the project, researchers led by Ben Raphael at Princeton University created an algorithm that quantifies the proportion of cancerous and non-cancerous cells in a tumour and investigates how these cells interact, which can also help discern how a tumour is growing.
Together, these discoveries bring us a step closer to understanding how cancer forms and evolves, which, in turn, could improve treatment. Abravanel says this could help in his clinical practice as well: “We try as best we can to match the right treatment to the right patient, but largely we aren’t able to, for individual cases, pull out what the best therapy would be at that moment in time.”
Topics:
[ad_2]
Source link

[ad_1]

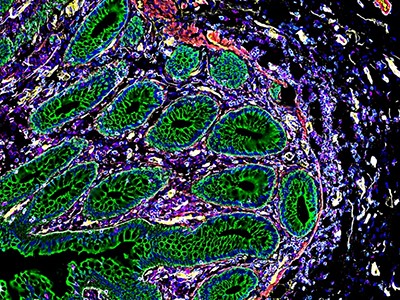
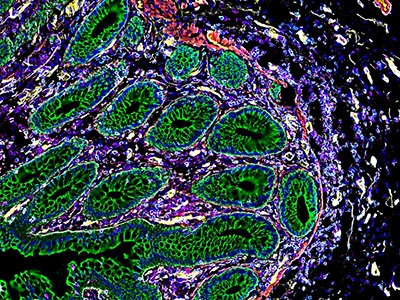
A large collection of papers maps the biology and locations of a range of cancer cells, including colon cancer (pictured).Credit: Steve Gschmeissner/Science Photo Library
Detailed maps that pinpoint the positions of cells in tumours and probe the tumours’ biology are offering insights into the development of several cancers — including in the breast, colon and pancreas — and could provide leads for potential treatments.
In a tranche of 12 papers published in Nature journals on 30 October, researchers of the Human Tumor Atlas Network (HTAN) analysed hundreds of thousands of cells from human and animal tissues. Some of the studies describe 3D maps of the cells — known as cell atlases — in tumours, whereas others create ‘molecular clocks’ that trace the cellular changes that lead to cancer.
“Applying these novel tools to cancer allow us to look at them with a different lens,” says Ken Lau, a computational cell biologist at Vanderbilt University Medical Center in Nashville, Tennessee, and co-author of a study that records the timing of cellular events in the development of colorectal cancer1. “We can actually see things that we couldn’t see before.”
In some of the studies, researchers created atlases that allowed them to study tumours at single-cell resolution and investigate how cancer begins. One team analysed the organization of cells in 131 samples of six types of cancer, including those of the breast, colon, pancreas and kidney2. The scientists found that distinct regions in the same tumour could respond differently to drugs. Understanding how various cancer-cell clusters respond to treatments could help researchers to design more effective ones.
Cell ‘atlases’ offer unprecedented view of placenta, intestines and kidneys
Other studies used 3D mapping to study samples of colon polyps — abnormal growths in the lining of the gut that can turn cancerous. They identified molecular changes in the polyps’ cells, including the loss of DNA connections and alterations in the activity of genes3, as well as changes in the immune response, cell growth and hormone metabolism4 that occur early on and could cause the polyp cells to turn cancerous.
Therapies that target these changes could make cancer treatments and early health interventions more effective, says Ömer Yilmaz, a stem-cell biologist at the Massachusetts Institute of Technology in Cambridge. “The best treatment for cancer is prevention. And if we can understand how different cell populations respond to the environment and to the diet, how that impacts tumour initiation and how different clones contribute to that process, it could lead to better prevention or detection methods.”
Other atlases offer clues about why some cancer types are more challenging to treat than others. “Tumours are not just composed of cancer cells,” says Daniel Abravanel, a physician–scientist at the Dana-Farber Cancer Institute in Boston, Massachusetts, and co-author of a study on breast cancer5. For instance, immunotherapies, which don’t target cancer cells directly but aim to help the immune system eliminate them, are less effective against breast cancer than other types, he adds.
To investigate why, Abravanel and his colleagues created a 3D tumour atlas using dozens of samples from 60 people with aggressive forms of breast cancer. They studied how immune cells are distributed and found that some types of immune cell were more common than others in certain tumours, especially in people who had received immunotherapy.

Why are so many young people getting cancer? What the data say
For three people, biopsies taken from the same tumour 70–220 days apart showed differences in the levels of immune cells known as T cells and macrophages. In two cases, the numbers of these cells had decreased over time, whereas in the third they had increased.
This “really shows how dynamic the immune microenvironment is, and it may explain why attempts to characterize tumours and predict responses to immune-checkpoint therapies from one biopsy at a single time point has had inconsistent results”, says Brian Lehmann, a breast-cancer researcher who specializes in genomics at the Vanderbilt-Ingram Cancer Center in Nashville, Tennessee.
In another study, researchers found that some aggressive subtypes of breast cancer had more immune cells than others, and seemed to become ‘worn out’ over time6. These cells expressed a protein called CTLA4, which limits their ability to respond to tumours. Therapies targeting CTLA4 have shown promising results in treating melanoma and lung cancer. “This opens up additional avenues for using that therapy in a subset of breast cancers,” says Lehmann.
Other experiments reveal insights into how cells turn cancerous in the first place. In the colorectal-cancer study, Lau and his colleagues engineered a ‘molecular clock’ to track how normal cells start to turn rogue and begin proliferating uncontrollably in the gut1. They used single-cell analysis and a gene-editing CRISPR tool to generate mutations in each cell’s DNA. These mutations acted as time stamps, recording the timeline of changes in and divisions of each cell.
The race to map the human body one cell at a time
Lau and his team applied this approach to 418 human colon polyps and found that up to 30% of the polyps originated from several cell types, rather than from a single cell. In 60% of the polyps, one group of cells started to ‘overtake’ others as the polyp grew — developing into a tumour. Two similar studies in mice7,8, including an analysis of 260,922 single cells from 112 samples of intestinal tissues, also found that a mix of cells collectively initiate colorectal tumours.
These findings overturn previous thinking that colon cancers arise from single rogue cells in the gut’s lining, and could open up opportunities for early diagnosis and intervention.
“To evaluate the risk of [pre-cancerous growths], what people use is the size. The larger the tumour, the more risk it has,” says Lau. But the molecular-clock and other analyses reveal that “there may be other biomarkers in terms of looking at genetics and evolution”.
[ad_2]
Source link

[ad_1]
Intricate molecular machineries, such as the ESCRT protein complexes, are well known for their ability to cut biological membranes. The discovery that membranes can also be severed by phase-separated condensates, through line tension force, reveals a previously unknown mechanism of membrane fission that highlights the fundamental role of condensates in cellular organization.
[ad_2]
Source link

[ad_1]
Haematopoietic stem cells from donors have been used to treat hundreds of thousands of people with blood cancer and other blood disorders.Credit: SPL
Ever since the first blood-forming stem cells were successfully transplanted into people with blood cancers more than 50 years ago, researchers have wondered whether they developed cancer-causing mutations. A unique study1 on the longest-lived transplant recipients and their donors has revealed that people who receive donor stem cells don’t seem to have an increased risk of developing such mutations.
The results are surprising but reassuring, says Michael Spencer Chapman, a haematologist at the Barts Cancer Institute in London.
“It’s fantastic news for people undergoing these therapies,” says Alejo Rodriguez-Fraticelli, a quantitative stem-cell biologist at the Institute for Research in Biomedicine in Barcelona, Spain.
Blood-forming, or ‘haematopoietic’, stem cells are precursor cells that reside in the bone marrow and give rise to all types of blood cell. They have been used to treat hundreds of thousands of people with blood cancers and bone-marrow diseases. The transplants involve depleting a person’s entire blood stem-cell reserves and replacing them with cells from a healthy donor. But researchers have long worried that putting the cells under such pressure could increase the risk of cancer. In rare cases, about 1 in every 1,000 transplants, donor cells develop into a cancer in the recipients.
The latest study, published in Science Translational Medicine this week, looked at mutations in specific genes that have been linked to cancer. It was thought that these mutations could give haematopoietic cells a growth advantage in transplant recipients, allowing them to rapidly divide and multiply as the recipient ages and eventually develop into leukaemia.
Some of the first transplants were conducted at the Fred Hutchinson Cancer Center starting in the late 1960s. In 2017, Masumi Ueda Oshima, a clinical researcher who studies post-transplant ageing at the Fred Hutchinson Cancer Center in Seattle, Washington, and her colleagues decided to reach out to the recipients of these transplants, and their donors, to collect samples of their blood and compare how the cells had aged. “It was really a big fishing expedition,” she says.
The team collected blood samples from 32 individuals — 16 donor–recipient pairs — who had received their transplants between 7 and 46 years ago. They used a highly sensitive technique to sequence genes known to acquire mutations associated with bone-marrow cancers.
The team found cells with mutations in all the healthy donors, even those as young as 12 years old. The older the donor, the mutations were present in their blood, but overall the frequency remained low — just one in a million of the sequenced base pairs.
The researchers then compared mutation patterns in 11 donor–recipient pairs for which they could access donor blood samples from the time of the transplant. They found similar mutation patterns in both groups. On average, mutations occurred at a rate of 2% per year in donors, and 2.6% per year in recipients. “Surprisingly, there actually are very few new mutations in the stem cells arising through the transplant process,” says Spencer Chapman. That suggests transplant recipients’ cells age at a similar rate to those in their donors, and they don’t have an increased risk of developing mutations, which might predispose them to blood cancers.
The fact that the mutations remain stable for so long after a transplant shows that “the regenerative capacity of the hematopoietic system is really profound”, says Ueda Oshima.
Rodriguez-Fraticelli says that although the results are comforting, they are based on a small number of individuals, which makes it difficult to draw broad conclusions.
Spencer Chapman observed similar results in a separate study of donor–recipient pairs2, which was been posted online as a preprint in April 2023. His study included 10 transplant recipients who received haematopoietic cells from their siblings between 9 and 31 years earlier. But they didn’t just look for changes in specific genes associated with cancer, instead they extracted and grew haematopoietic cells in a dish and sequenced the entire genomes of individual cells. On average, they found that recipients had only slightly more mutations than their donors, adding just 1.5 years of normal ageing — a similar finding to Ueda Oshima’s.
When he and his colleagues looked specifically at mutations known to give cells a growth advantage, they noticed that cells that had only one of these mutations were found at similar levels in recipients and donors. But cells with two or more of these advantageous mutations were present at higher levels in recipients than donors. The result could help to explain why in rare cases, transplanted cells can develop into tumours.
But more work is needed to better understand the implications of these ageing processes, in terms of cancer risk and immune function, says Spencer Chapman.
Both studies could have implications for people receiving stem-cell transplants and blood-based gene therapies to treat sickle-cell disease, for example. More of these therapies are “hitting the mainstream” and being given to children, who will need to rely on the transplanted cells for the rest of their lives, says Spencer Chapman.
[ad_2]
Source link
[ad_1]
A woman with type 1 diabetes started producing insulin (blue) after a stem cell transplant.Credit: Lennart Nilsson, Boehringer Ingelheim International GmbH, TT/Science Photo Library
A 25-year-old woman with type 1 diabetes started producing her own insulin less than three months after receiving a transplant of reprogrammed stem cells1. She is the first person with the disease to be treated using cells that were extracted from her own body.
“I can eat sugar now,” said the woman, who lives in Tianjing, on a call with Nature. It has been more than a year since the transplant, and, she says, “I enjoy eating everything — especially hotpot.” The woman asked to remain anonymous to protect her privacy.
James Shapiro, a transplant surgeon and researcher at the University of Alberta in Edmonton, Canada, says the results of the surgery are stunning. “They’ve completely reversed diabetes in the patient, who was requiring substantial amounts of insulin beforehand.”
The study, published in Cell today, follows results from a separate group in Shanghai, China, who reported in April that they had successfully transplanted insulin-producing islets into the liver of a 59-year-old man with type 2 diabetes2. The islets were also derived from reprogrammed stem cells taken from the man’s own body and he has since stopped taking insulin.
The studies are among a handful of pioneering trials using stem cells to treat diabetes, which affects close to half a billion people worldwide. Most of them have type 2 diabetes, in which the body doesn’t produce enough insulin or its ability to use the hormone diminishes. In type 1 diabetes, the immune system attacks islet cells in the pancreas.
Islet transplants can treat the disease, but there aren’t enough donors to meet the growing demand, and recipients must use immune-suppressing drugs to prevent the body from rejecting the donor tissue.
Stem cells can be used to grow any tissue in the body and can be cultured indefinitely in the laboratory, which means they potentially offer a limitless source of pancreatic tissue. By using tissue made from a person’s own cells, researchers also hope to avoid the need for immunosuppressants.
In the first trial of its kind, Deng Hongkui, a cell biologist at Peking University in Beijing, and his colleagues extracted cells from three people with type 1 diabetes and reverted them into a pluripotent state, from which they could be moulded into any cell type in the body. This reprogramming technique was first developed by Shinya Yamanaka at Kyoto University in Japan almost two decades ago. But Deng and his colleagues modified the technique3: instead of introducing proteins that trigger gene expression, as Yamanaka had done, they exposed the cells to small molecules. This offered more control over the process.
The researchers then used the chemically induced pluripotent stem (iPS) cells to generate 3D clusters of islets. They tested the safety and efficacy of the cells in mice and non-human primates.
In June 2023, in an operation that lasted less than half an hour, they injected the equivalent of roughly 1.5 million islets into the woman’s abdominal muscles — a new site for islet transplants. Most islet transplants are injected into the liver, where the cells cannot be observed. But by placing them in the abdomen, the researchers could monitor the cells using magnetic resonance imaging, and potentially remove them if needed.
Two-and-a-half months later, the woman was producing enough insulin to live without needing top-ups, and she has sustained that level of production for more than a year. By that time, the woman had stopped experiencing the dangerous spikes and drops in blood glucose levels, which remained within a target range for more than 98% of the day. “That’s remarkable,” says Daisuke Yabe, a diabetes researcher at Kyoto University. “If this is applicable to other patients, it’s going to be wonderful.”
The results are intriguing, but they need to be replicated in more people, says Jay Skyler, an endocrinologist at the University of Miami, Florida, who studies type 1 diabetes. Skyler also wants to see that the woman’s cells continue to produce insulin for up to five years, before considering her ‘cured’.
Deng says the results for the other two participants are “also very positive”, and they will reach the one-year mark in November, after which he hopes to expand the trial to another 10 or 20 individuals.
Because the woman was already receiving immunosuppressants for a previous liver transplant, the researchers could not assess whether the iPS cells reduced the risk of rejection of the graft.
Even if the body doesn’t reject the transplant because it doesn’t consider the cells to be ‘foreign’, in people with type 1 diabetes, because they have an autoimmune condition, there is still a risk that the body could attack the islets. Deng says they didn’t see this in the woman because of the immunosuppressants, but they are trying to develop cells that can evade this autoimmune response.
Transplants using the recipient’s own cells have advantages, but the procedures are difficult to scale up and commercialize, say researchers. Several groups have started trials of islet cells created using donor stem cells.
Preliminary results for one trial, led by Vertex Pharmaceuticals in Boston, Massachusetts, were reported in June. A dozen participants with type 1 diabetes received islets derived from donated embryonic stem cells that were injected into the liver. They were all treated with immunosuppressants. Three months after the transplant, all the participants began producing insulin when glucose was present in their bloodstreams4. Some had become insulin independent.
Last year, Vertex launched another trial in which islet cells derived from donated stem cells were placed in a device designed to protect them from immune-system attacks. It was transplanted into a person with type 1 diabetes, who did not receive immunosuppressants. “That trial is ongoing,” says Shapiro, who is involved in the study, which aims to enrol 17 individuals.
Yabe is also about to start a trial using islet cells produced using donor iPS cells. He plans to develop sheets of islets and surgically place them in the abdominal tissue of three people with type 1 diabetes, who will receive immunosuppressants. The first participant should receive their transplant early next year.
[ad_2]
Source link

[ad_1]

NASA astronauts Sunita Williams and Butch Wilmore are stuck on the ISS for months because of technical issues with Boeing’s Starliner spacecraft.Credit: NASA via AP/Alamy
Over the course of just one month in space, engineered human heart tissue got weaker, its ‘beating’ patterns became irregular and it underwent molecular and genetic changes that mimicked the effect of ageing1. The findings are published in the Proceedings of the National Academy of Sciences today.
The study offers a useful means of identifying the molecular pathways behind the detrimental effects of spaceflight on the human heart, says Joseph Wu, a cardiologist at Stanford University in California.
Microgravity can be hard on the body, and astronauts exposed to it have experienced cardiovascular changes, such as an irregular heartbeat. But unpicking the effects on the heart of long-duration spaceflight — that lasting for months at a time — and the molecular changes that underpin those changes has remained out of reach, says study co-author Deok-Ho Kim, a biomedical engineer at Johns Hopkins University in Baltimore, Maryland. “It’s not possible to do the different molecular and functional studies in human astronauts,” he says.
To overcome this challenge, Kim and his colleagues sent engineered heart tissue to the International Space Station (ISS) for 30 days.
To engineer the tissue, the researchers coaxed human induced pluripotent stem cells — which act as blank canvases that can differentiate into any cell type — to develop into human heart muscle cells. The team then strung sets of six tissue samples between pairs of posts. One post in each pair was flexible, allowing the samples to contract like a beating heart. The system, which they call a heart-on-a-chip, was housed in a chamber about half the size of a cellphone.
Once the heart-on-a-chip system was on board the ISS, Kim and his colleagues used sensors to monitor the strength of the tissues’ contraction and beating patterns in real time. For comparison, they monitored another set of tissue samples that remained on Earth.
After 12 days on the ISS, the tissues’ contraction strength had almost halved, whereas that of their on-ground counterparts had remained relatively stable. This weakening was still apparent even after nine days of recovery back on Earth. In space, the tissues’ beats also became more irregular over time, with the period between each beat increasing by more than five times at day 19. But this irregularity disappeared after the samples came back to Earth. This suggests that NASA astronauts Sunita Williams and Butch Wilmore — who have been stuck on the ISS for months owing to technical problems with Boeing’s Starliner spacecraft — are probably experiencing cardiovascular stress that will resolve after they return to Earth, say Wu.
After getting the tissues back from space, Kim and his colleagues used transmission electron microscopy to look at the samples’ sarcomeres — strands of proteins responsible for muscle contractions. After being in orbit for a month, these protein bundles had become shorter and more disordered compared with those in the tissues that had remained on the ground. The mitochondria — the energy-producing machinery inside cells — had also become swollen and fragmented.
When the researchers sequenced the tissue samples’ RNA, they found an increase in the expression of genes and signalling pathways associated with inflammation and heart disorders in tissues that had travelled on the ISS. Meanwhile, genes that produce proteins required for normal heart contraction and mitochondrial function showed signs of reduced expression.
Although the study’s heart-on-a-chip approach is innovative, it doesn’t capture other important cardiovascular changes that can occur in the human heart, such as pressure in the arteries, says Wu. But he adds that a similar set-up could be useful for studying how other organs fare under microgravity and harsh radiation levels. “The platform’s ability to function in a microgravity setting whilst maintaining tissue viability is a major advantage,” he says.
Kim and his colleagues are planning to send other heart and organ tissues into space for a longer period to investigate the effects of spaceflight more deeply. They also hope to test drugs that can counteract some of the impacts of microgravity on the heart.
[ad_2]
Source link
[ad_1]
The problem of cell type became clear to genome biologist Jason Buenrostro in 2013. He was studying a cell line derived from someone with cancer, trying to map out how the DNA was arranged in the nucleus. The cells should have been pretty much identical, he thought. But the more Buenrostro looked at the DNA, the more differences he found in how it was packaged1. “I realized that there were probably hundreds of flavours,” recalls Buenrostro, who was a graduate student at Stanford University in California at the time.
This and other research pushed him to conclude that “every cell is a special snowflake”. And that conclusion significantly complicated his research into how some cancer cells develop resistance to drugs. For Buenrostro, now at Harvard University in Cambridge, Massachusetts, it meant that “all of these snowflake cells can actually be important”.
Despite their individuality, there are pragmatic reasons to group similar cells together. “Defining cell types is crucial for understanding new biological phenomena, elucidating underlying mechanisms, and identifying therapy targets,” says Zhang Zhang, a bioinformaticist at the Beijing Institute of Genomics at the Chinese Academy of Sciences.
Already, projects to build huge atlases of cells are yielding torrents of data and insights into disease. Since the mid-2010s, scientists categorizing cells have leant heavily on single-cell RNA sequencing, a technique that identifies the genes that each cell has turned on, to group those with similar profiles. The multinational collaboration, the Human Cell Atlas, launched in 2016, has analysed more than 90 million cells from more than 11,000 people in an ongoing effort to build 18 different atlases, and published more than 440 studies.
Cell ‘atlases’ offer unprecedented view of placenta, intestines and kidneys
But behind this progress lies a deceptively simple question: what exactly is a cell type?
“A cell type is a group of cells that are similar to each other and distinct from other groups of cells,” offers neuroscientist Hongkui Zeng, director of the Allen Institute for Brain Science in Seattle, Washington. But even that definition leaves plenty of room for interpretation: similar how? Distinct in what way?
Ask a dozen researchers and you’ll get as many different answers. In fact, when the journal Cell Systems did that in 2017, 15 researchers offered wildly different suggestions, pointing to developmental history, molecular profile, shape or function as possible identifiers2. “The debates can be quite heated,” says Buenrostro.
Perhaps that’s because the question goes to the heart of how scientists conceive of the basic unit of life. Some researchers reject the view that a cell is a simple summation of gene expression, as atlases based on RNA sequencing imply. Others argue that a cell’s progression through various states over time must also be considered.
But most can agree on one thing, says Barbara Treutlein, a multicellular systems biologist at the Swiss Federal Institute of Technology (ETH) in Zurich. “There’s a general consensus that it is extremely complicated.”
Such struggles over central definitions are hardly unique to cell biology: taxonomists have wrestled with ‘what is a species?’ for centuries, and geneticists had to confront ‘what is a gene?’ when the dogma of one gene making one protein began to break down decades ago.
Throughout the history of cell biology, cellular parts lists have appeared in many forms, reflecting the predominant technology of the time. Around 1900, microscopy was king, and researchers such as Spanish histologist Santiago Ramón y Cajal sketched cells and started grouping them by appearance. For example, certain common, stellate brain cells were called astrocytes, or star-like cells.
As a result of the molecular-biology revolution, which picked up steam in the mid-1900s, scientists learnt to classify cells on the basis of a limited set of molecular markers. So astrocytes became cells that produced glial fibrillary acid protein, or GFAP, which is easily visualized by staining cells with antibodies or tagging the GFAP gene with green fluorescent protein.
Then came single-cell RNA sequencing, a method3 first published in 2009. Today, cell cartographers might define astrocytes by the host of RNAs that they express — an approach that has parallels with the use of comparative genomics to understand the evolution of species.
But none of those tools says much about what astrocytes do, which is to support neurons and synapses.

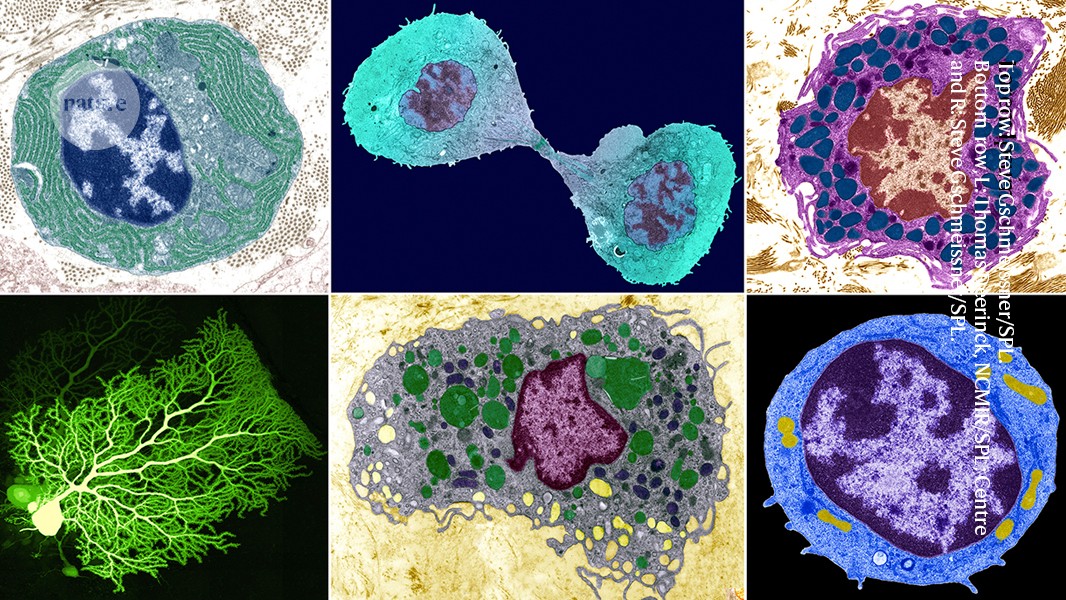
Purkinje neurons (turquoise) in the cerebellum, a brain area that controls movement and other functions.Credit: Thomas Deerinck, NCMIR/Science Photo Library
Not that trying to group cells by function is easy. One class of cell that has often been categorized in a functional manner is neurons, which are frequently classified by the chemicals — such as dopamine or serotonin — that they release, says Anne West, a neurobiologist at Duke University in Durham, North Carolina. But many neurons make the same neurotransmitters; for example, scientists in the mid-2000s debated how many types of interneuron produced the neurotransmitter GABA; estimates ranged from four to many, many more. West expects ongoing work with single cells and RNA expression across the brain will help the field to agree on a number.
Nonetheless, cell function might be, “in principle”, the best way to define a cell type, says Joshua Sanes, a neurobiologist at Harvard. And part of a cell’s function, Treutlein adds, is its response to its environment. In living tissue, cells are constantly exposed to signals that could influence them, such as metabolites, hormones or pathogens. “You only really know what type a cell is once you also know how it responds,” Treutlein says. “These states, all together, will tell you what it is.”
She suggests that a future phase of cell atlases should include how cells respond to such changes — for instance, how cells might alter their developmental trajectories in response to drug treatments.
Unfortunately, cell responses and functions are not obvious for many cell types, and might be transient features. Working them out is time-consuming, and cells often change function when transferred from an entire organism into a laboratory dish for focused study.
This forces researchers to adopt more practical cell-typing criteria and explains the dominance of standardized molecular methods — mainly single-cell RNA sequencing, but also the technique developed by Buenrostro and others to examine how DNA is packaged4, as well as spatial methods that link these molecular markers to a cell’s place in tissues. By combining those approaches, “we’ve really redefined what cell types are”, says Sarah Teichmann, a genome biologist and biophysicist at the University of Cambridge, UK, and co-chair of the Human Cell Atlas project.
This new molecular approach has yielded exciting results that promise to rewrite much of what cell biologists know about the body. Indeed, although scientists once estimated that there were about 200 cell types in the human body, last year Zeng and her colleagues identified more than 5,000 RNA-based clusters — and therefore potential cell types — in the cortex of the mouse brain alone5.
Focused efforts are also turning up new types, even in well-explored tissues. For example, about 10 years ago, Sanes and his colleagues began investigating the cell types in the mouse retina with single-cell RNA sequencing. At the time, scientists had estimated that there were about 65; the new analysis6 netted at least 130. Before that, researchers had probably missed rarer types or very similar ones that the molecular methods could distinguish, Sanes suggests. Sanes and his collaborators are now comparing retina atlases from different species7.
This is the largest map of the human brain ever made
Cell atlases directly affect medical investigations, too. Two independent research teams discovered a rare, new cell type, that is potentially involved in cystic fibrosis8,9; another group profiled and mapped pacemaker cells in the heart10.
During the COVID-19 pandemic, many atlas researchers turned to investigations of the virus SARS-CoV-2, says Aviv Regev, a computational and systems biologist and head of research and early development at biotechnology company Genentech in South San Francisco, California, who co-chairs the Human Cell Atlas. Studies identified a variety of cell types that were susceptible to infection and showed how their cellular responses mirrored or diverged from those in other diseases11.
Regev says that Genentech is already using cell-atlas data in drug development. For example, one team has been testing a drug for lung disease that binds to a receptor found in cells in the lung. But perusing the cell atlas, the researchers discovered the same receptor in more cells located in the gut that are relevant to inflammatory bowel disease. This led them to test the same drug for that condition. Without the resource, they never would have noticed the similarity, says Regev.
Beyond the quest for therapies and the desire to make an inventory of the body, the cell-type question speaks to a deeper quandary: what is the basic unit of life?
“I would say broadly there are two camps,” says Itai Yanai, a systems biologist at New York University Langone Health. “One camp looks at cells, and the other camp looks at genes.”
One person firmly in the cell-focused camp is Alfonso Martinez Arias, a developmental biologist at the Catalan Institution for Research and Advanced Studies in Barcelona, Spain. He says that single-cell RNA sequencing creates a gene-centric view that distracts scientists from other questions. “I think a cell is much more than the sum total of the RNAs that it contains,” says Martinez Arias. For example, when he grows cells in a dish to model the early embryo, the RNA profiles of 2D cultures differ little from those of 3D organoids, he says — even though the 3D versions have very different structures and organizations.
For scientists such as Yanai, however, genes are the fundamental unit of life, and cells are manifestations of those genes. So cataloguing cell type by RNA makes sense: “You tell me which genes are on, I’ll tell you what cell type,” he says. For example, he says, the skin’s pigment-making cells, melanocytes, express a particular “melanocyte module” of genes.

Villi in the small intestine, which help to absorb nutrients from food.Credit: Thomas Deerinck, NCMIR/Science Photo Library
Another rubric for defining cell type, says Yanai, is to look at the physical state of the genome in the nucleus — how the genome forms loops and coils, leaving some genes accessible and others sequestered, and governing which genes are available for transcription.
But even that genomic arrangement is controlled by other upstream genes and proteins. Could those regulatory molecules be considered the true root of cell types? Günter Wagner, an evolutionary biologist at the University of Vienna, Austria, thinks so.
Wagner and his colleagues have a theory12: that cell types are controlled by large complexes of transcription factors and other molecules called the ‘core regulatory complex’, or CoRC. This big ball of collaborating regulators would pluck the DNA strings to turn on some genes and suppress others, and therefore determine chromatin arrangement, RNA profile — and cell type. CoRCs have been defined for a handful of cell types, such as neural and blood cells, says Wagner, but it’s not clear yet how generalizable the concept is. He suspects that CoRCs would define a shorter list of cell types than would clusters based on single-cell analyses.
The CoRC “is kind of like the unicorn that you’re searching for, for what a cell type is”, says Jeff Doyle, a plant systematist at Cornell University in Ithaca, New York. He has seen hints of them in some plant-cell atlases.
As for the current focus on RNA sequencing, Teichmann admits that the critics have a point. “Of course, a cell type isn’t just the RNA profile,” she says. She notes that the Human Cell Atlas expects to incorporate different methods of cell typing; RNA analysis was just the first to become manageable at scale. And she says that it’s been powerful because RNA reflects other aspects of a cell’s biology, including the arrangement of chromatin and its complement of proteins.
Cell types are often sketched according to a cell’s present identity. But a cell’s past and future are just as crucial, says Sam Morris, a stem-cell biologist at Washington University School of Medicine in St. Louis, Missouri. Even cells with seemingly stable identities might have the potential to turn into different types — such as an immune cell that activates to fight infection — or even turn cancerous or diseased under some conditions.
A cell’s past, of course, is of deep interest to developmental biologists, who study how one cell divides and diversifies to produce first an embryo and then an entire creature. That’s why the ultimate representation of cell types should be a tree-like structure, rooted in the body’s first cell and ending with mature types at the branch tips, argues Jay Shendure, a developmental geneticist at the University of Washington in Seattle. A parts list in an atlas, he says, “under-prioritizes the concept of time and the notion of continuity”.
The Human Cell Atlas: from vision to reality
Researchers are beginning to create the data that would underlie such trees. For example, in a study this year, Shendure and his colleagues tracked single-cell transcriptomes in mouse embryos from early development to birth and beyond. They found major changes in the RNA that was expressed in cells during the hour after birth, probably because the animals had to adapt to life outside the womb13.
Tracking cell types by developmental lineage has its own problems, however. There are rare instances when types that seem identical can arise through different trajectories. And it’s not clear yet how to categorize intermediate forms. “I still think there’s a question of, is cell identity a continuous property, is it a discrete property?” says Morris.
There’s also a more transient cellular property, called cell state, to consider. A cell’s type can remain consistent while its state radically changes: say, from newly born to preparing for the next cell division, or from quiescent to activated. It can be very challenging to distinguish impermanent cell states from true cell types, says Zhang.
If different technologies don’t classify cells in the same way, and every cell is an individual at the finest level, then what is a cell type?
If the concept still seems vague, that’s as it should be, argues Allon Klein, a systems biologist at Harvard Medical School in Boston, Massachusetts. He says that the concept can be both “extremely useful and poorly defined” at the same time.
That’s because ultimately, there’s no simple ground truth to find. Nature hasn’t created a neat parts list as a human engineer would, and any effort to delineate categories is in some sense artificial. The same is true of taxonomists’ efforts to define species: the question never really went away, says Klein, but the answers evolved as genetic data poured in. Klein thinks that something similar will happen in cell biology.
Researchers are already coming up with more nuanced ways to accept and account for cellular variation. Buenrostro and Regev have come to see cells less as members of a particular type, and more as collections of identities, based on the modules or pathways that a given cell is running at a given time. So a cell could be running, say, a stable ‘fibroblast’ program with overlay states of ‘activate to repair wound’ and ‘cell division’.
The modules that matter to a given researcher will depend on their interests and perspective. That’s why the metaphor of a cell ‘atlas’ is so fitting, says Regev. Just like a geographical atlas combines natural features, political borders and other concepts, cell atlases can also unify different versions of cell identity — no matter the user’s perspective, or where they are headed.
[ad_2]
Source link
[ad_1]
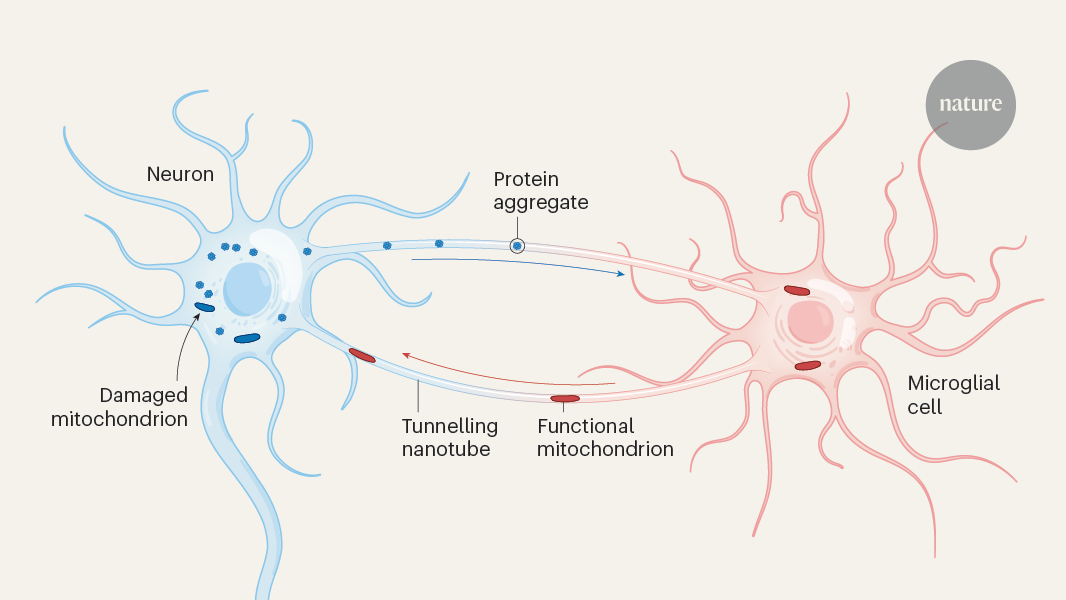
Nature, Published online: 11 September 2024; doi:10.1038/d41586-024-02862-z
Tiny cellular tubes between neurons and brain cells called microglia serve as conduits for the export of toxic protein aggregates from neurons and the import of healthy organelles, keeping neurodegeneration at bay.
[ad_2]
Source link