[ad_1]
Nature, Published online: 20 November 2024; doi:10.1038/d41586-024-03824-1
Can jets of drugs from pressurized capsules replace needles?
[ad_2]
Source link

[ad_1]
Nature, Published online: 20 November 2024; doi:10.1038/d41586-024-03824-1
Can jets of drugs from pressurized capsules replace needles?
[ad_2]
Source link

[ad_1]

Researcher Yan Zeng looks over the machinery at the A-Lab, a fully automated laboratory at the Lawrence Berkeley National Laboratory in California.Credit: Marilyn Sargent/Berkeley Lab
Stephan Noack’s official title is bioprocess engineer. In simple terms, he is a problem-solver. His colleagues at the Jülich Research Centre in Germany knock on his office door armed with some of their thorniest questions about the process of coaxing bacteria, algae and other microbes into mass-producing valuable chemicals, such as ethanol and amino acids. Optimizing such processes requires making tiny adjustments to several variables, including the microbes’ food source and growing temperature. It’s trial and error — mostly error. “During the set-up of these workflows, a lot of failure happens,” Noack says.
Even the most efficient laboratories, with an ample amount of students to conduct the trials, can fail to complete the lengthy, laborious process. “It was a huge bottleneck,” he says. Noack and his engineers have therefore been turning to robotics and automation to speed up the process of growing microorganisms on plates of gelatinous agar. By combining a range of equipment, from robotic arms to liquid handlers, researchers have been able to swap out large single plates of agar for ones containing 96 or 384 tiny wells. This has increased throughput nearly 100-fold according to Noack.
Nature Outlook: Robotics and artificial intelligence
Although they are common in large industrial research facilities, robotics and automation have only begun to trickle down into smaller academic labs in the past five years, says Ian Holland, a postdoctoral researcher at the University of Edinburgh, UK. Historically, he says, academia has relied on large populations of students and postdocs to do the time-consuming work. But with scientific advances requiring ever-increasing amounts of data generation and analysis, lab workers can’t work quickly enough. But robots can.
The advances include robotic arms that can pipette more accurately than can human scientists1 and fully automated ‘cloud’ labs that experimenters can access online and command a robot workforce to perform their instructions from anywhere in the world2. Researchers who are leaning towards automation hope that the shift will decrease cost, save time and generate fewer errors while improving reproducibility.
But these changes don’t come without challenges. Scientists need a deep understanding of their experiments to program machinery and to prevent the propagation of errors. The equipment can be expensive and require hours of labour to fix and maintain. If done correctly, however, laboratory automation can transform science, according to Dennis Knobbe, a roboticist at the Technical University of Munich in Germany. “It’s not about excluding the human from these processes,” Knobbe says. “It’s instead about using robotics to enhance researchers’ capabilities.”
In 2012, Matheus Carvalho, a research technician and fisheries biologist at the Southern Cross University in Lismore, Australia, encountered AutoIt, a programming language originally created for automating Microsoft Windows tasks. Around the same time, he came across a toy robotic arm that could be controlled through a computer. Carvalho reasoned that if he could combine the toy robot with AutoIt, he could automate some of his tedious sampling tasks in the lab. Although the first robotic arm broke almost immediately, Carvalho convinced his supervisor to purchase a higher-quality, second-hand arm, which was built into an automated sampling machine that continues to operate more than a decade later. Carvalho was quickly sold on the idea of laboratory automation, which is the topic of a book he published in 2017.

Matheus Carvalho at the Southern Cross University in Lismore, Australia, created an automated sampling machine using a reprogrammed toy robotic arm.Credit: Matheus Carvalho de Carvalho
He aimed to automate more lab procedures without precluding human involvement. His lab used non-radioactive isotopes to understand organic material in water samples — a process that requires weighing and measuring tiny amounts of powders, often to a fraction of a milligram. Every powder they tested had a different grain size and texture, which made it impossible to program a robot to measure out all the samples. Instead, Carvalho devised a protocol that allowed people and machines to each do what they were best at: a human lab technician weighed out the powder samples, and a small, mobile robot was programmed to retrieve containers and calibrate the scales. “It’s better to automate what is easy but leave the hard parts for us humans,” Carvalho says.
In the 2010s, Dina Zielinski, who was then a technician at the Whitehead Institute in Cambridge, Massachusetts, faced similar challenges with automation while working on a different type of test. She wanted to sequence tissue samples from people with Parkinson’s disease to understand the genes contributing to the condition. The job required pipetting — a lot of pipetting. Zielinski saw the task in front of her as a fast track to repetitive strain injury.
“Molecular biology essentially entails combining minuscule clear volumes with other miniscule clear volumes,” Zielinski says. “If you didn’t combine the right tiny volumes, you would have wasted a ton of money on sequencing.”
Even worse, she says, these samples were rare and hard to obtain. Yaniv Erlich, who was then a principal investigator, and his late collaborator Susan Lindquist, a biomedical researcher at the Whitehead Institute, began investigating various robotics, including automated liquid handlers, to speed up the process and to save Zielinski’s hands from injury. But none of the robots they investigated could provide both the precision and flexibility that the lab needed. So, Zielinski, Lindquist and Erlich, who is now chief executive of Eleven Therapeutics in Cambridge, UK, decided to build something different.

The iPipet app can be used to illuminate sections of a 96-well plate and help researchers to ensure they combine the correct samples.Credit: Dina Zielinski
The idea they came up with didn’t handle the pipetting itself. Instead, the team built an iPad app that users could program to help them pipette the correct samples into the correct position. The iPipet app illuminates sections of 96- or 384-well plates to enable a scientist to ensure they combine the correct samples3. When Zielinski pitted a researcher using iPipet against a top-of-the-line robot, the app-assisted human was the clear winner. “The error was much lower with human pipetting than with the liquid-handling robot,” she says.
What makes efforts such as these so trailblazing isn’t their complexity but rather their simplicity. The goal is to find a middle ground between the expensive instruments that can perform every aspect of an experiment and the labour of a single student performing all their tasks manually, Holland says. Ideally, such technology would make it possible for researchers to spend time planning experiments and analysing results instead of pipetting samples.
“If automation can take some of the load off you, you can do more things and be a better researcher,” Holland says. And the academic environment is well-suited for this melding of human and machine. “You’ve got engineering students looking for projects and we’ve got biologists who have problems that need solving.”
However, the changes come at a cost says Holland. Since the dawn of the industrial revolution, people have invested time, resources and money into developing machinery to make products more quickly and cheaply. In commercial settings the benefits were clear, says Holland — investment in automation paid off because it allowed production of more commodities with low labour costs.
Academia is different. Industry focuses on profit, whereas academic labs place a greater emphasis on training the next generation of scientists and producing knowledge. A steady flow of students who are willing to work long hours — some of whom have their own grants and stipends as salary — means that labour costs aren’t as important. What’s more, the focus on teaching and training means that many scientists have conventionally seen automation as anathema to their mission as educators.

Postdoc researcher Julia Tenhaef and bioprocess engineer Stephan Noack at the Jülich Research Centre in Germany use an automated laboratory system called the AutoBioTech platform. Credit: Stephan NoackCredit: Stephan Noack
“In academia, you could spend US$100,000 on this machine, but it’s only going to make your output a bit faster,” says Holland. “That’s a lot harder to justify.” As a result, many academic labs have much less robotic equipment than do commercial and industrial labs — something Holland refers to as the automation gap4.
Joshua Pearce faced down these technological costs when he founded his lab at Michigan Technological University in Houghton in the mid-2000s. Now an engineer at Western University in London, Canada, Pearce was developing methods to build better photovoltaic systems to generate electricity from sunlight. He wanted to improve solar cells’ ability to absorb different wavelengths of light, but the automated filter wheel changer, which adjusted the wavelengths on his custom-built machine, broke. The replacement was $2,500 (an exorbitant price for a simple part) and had a five-month lead time.
Pearce realized that he was at a university filled with budding engineers, so he hired some students to help him 3D print the necessary components. What resulted was a bespoke device crafted entirely from open-source hardware and software that cost $50 and did exactly what Pearce needed it to. “It was something that wasn’t available on the market,” Pearce says. “You can make really high-end equipment, exactly what you want, and do it fairly easily for extremely low cost.”
With his equipment that could automatically adjust light wavelengths for his tests, Pearce began campaigning about the potential of open-source design as a cost-effective way to reap the benefits of lab automation5. He is now editor-in-chief of the journal HardwareX, a publication that allows researchers to share their code and blueprints — while also helping to bolster their CVs and tenure qualifications.
Pearce’s experiences challenge the idea that investing in automation hampers a scientist’s ability to train students, along with the opinion that robotics are prohibitively expensive.
When it comes to the future of lab robotics, Knobbe thinks that inventions such as those created by Pearce, Carvalho and Zielinski will be key: modular, multipurpose and budget-friendly. “We don’t want to just build a huge machine, like an encapsulated system,” Knobbe says. “We want to integrate these robotic systems into everyday laboratories.”
He also imagines fully fledged robotic lab assistants that can perform basic experimental tasks with minimal supervision. Although this technology is nowhere near ready, Knobbe says, he thinks researchers will be able to deploy modular automated systems that can interact with each other and be controlled by a robotic assistant in the next ten years. One of the biggest challenges will be balancing robustness, flexibility, the ability to detect errors and asking for help.
Building or buying a top-of-the-line machine that only does pipetting would force lab technicians to work around the machine. Knobbe wanted a robot that would work with his team, follow basic commands and scan the environment for obstacles. He is therefore building a robotic pipette with finger-like appendages. Early testing shows that this machine has met industry standards, he says.
Although reducing variability and mistakes has long been one of the selling points of robotics and automation, Knobbe says that robots can also propagate errors1,4. Knobbe also speculates that robots might create types of catastrophic failure.
A cautionary tale emerged in November last year, when a team of scientists from Google DeepMind in London, the University of California, Berkeley, and the Lawrence Berkeley National Laboratory in California teamed up to predict nearly 400,000 new compounds using artificial intelligence (AI) and then to synthesize these compounds in a fully automated laboratory, called A-Lab. The project was an endeavour to identify new high-performance, low-cost materials by automating both the physical synthesis of compounds and their subsequent analysis. A resulting Nature paper6 seemed to showcase the benefits of automation.
“It was a high-risk, high-reward project,” says co-author Yan Zeng, a former researcher at the Lawrence Berkeley National Laboratory who started her own lab at Florida State University in Tallahassee this year. “It was a little bit crazy, to be fully automated.”
Several weeks later, however, some scientists began raising questions about the AI’s ability to predict truly new materials. What seemed to be new in the computer’s modelling might have been different versions of known compounds. “This paper did not at all live up to its claims,” says Leslie Schoop, a chemist at Princeton University in New Jersey.
To Zeng, however, the study was as much about the process — demonstrating how such a system could be built, operated and used by materials scientists — as it was about the results. In fact, Zeng says, the robotic synthesis aspects of the study performed exactly as expected. She concedes that the initial programming steps took months and required a team of technicians to troubleshoot the process. But they quickly recouped the lost time as the robots required minimal human contact.
Zeng is now working to automate parts of her lab in Florida. Her first target is hydrothermal synthesis — a process that requires high temperatures and pressurized tubes. It’s a complex project, but her time at Berkeley gave her valuable experience in breaking down complex robotics into more manageable steps, and she hopes to begin automating this process as she scales up her lab.
Despite the scepticism over A-Lab, she remains optimistic about automation. Robotics could provide the key to future breakthroughs, she says, equipping researchers with the freedom and flexibility to think up the experiments of tomorrow. “This is a rising field, and it’s rising up pretty fast,” says Zeng.
[ad_2]
Source link

[ad_1]
Nogueiras, R., Nauck, M. A. & Tschöp, M. H. Nature Metab. 5, 933–944 (2023).
Christoffersen, B. Ø. et al. Obesity 30, 841–857 (2022).
Sass, F. et al. Nature https://doi.org/10.1038/s41586-024-08207-0 (2024).
Wilding, J. P. H. et al. N. Engl. J. Med. 384, 989–1002 (2021).
Jastreboff, A. M. et al. N. Engl. J. Med. 387, 205–216 (2022).
Lecci, A., Capriati, A. & Maggi, C. A. Br. J. Pharmacol. 141, 1249–1263 (2004).
Ebner, K., Sartori, S. B. & Singewald, N. Curr. Pharmaceut. Des. 15, 1647–1674 (2009).
Pontzer, H. et al. Science 373, 808–812 (2021).
[ad_2]
Source link

[ad_1]
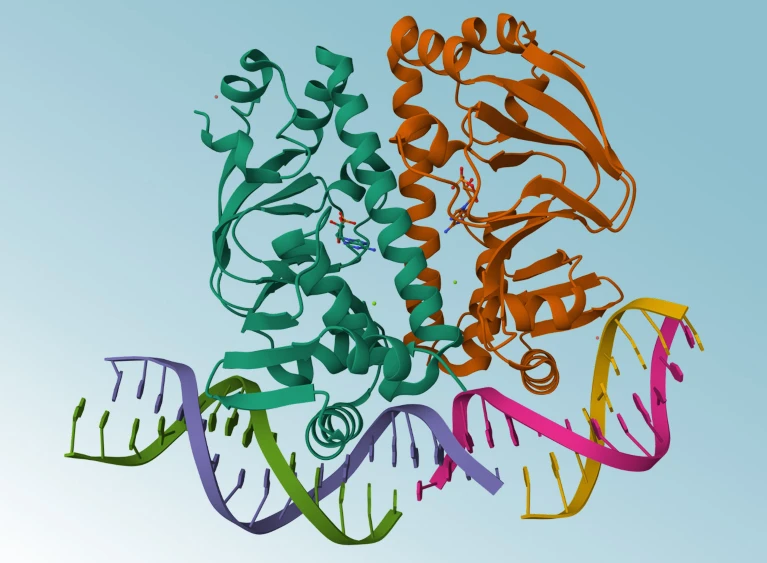
AlphaFold3 can predict the structures of proteins as they interact with DNA.Credit: Werel et al./American Society for Microbiology, Mol*, RCSB PDB
AlphaFold3 is open at last. Six months after Google DeepMind controversially withheld code from a paper describing the protein-structure prediction model, scientists can now download the software code and use the artificial intelligence (AI) tool for non-commercial applications, the London-based company announced on 11 November.
“We’re very excited to see what people do with this,” says John Jumper, who leads the AlphaFold team at DeepMind and last month, along with CEO Demis Hassabis, won a share of the 2024 Chemistry Nobel Prize for their work on the AI tool.
Major AlphaFold upgrade offers boost for drug discovery
AlphaFold3, unlike its predecessors, is capable of modelling proteins in concert with other molecules. But instead of releasing its underlying code — as was done with AlphaFold2 — DeepMind provided access via a web server that restricted the number and types of predictions scientists could make.
Crucially, the AlphaFold3 server prevented scientists from predicting how proteins behave in the presence of potential drugs. But now, DeepMind’s decision to release the code means academic scientists can predict such interactions by running the model themselves.
The company initially said that making AlphaFold3 available only through a web server struck the right balance between enabling access for research and protecting commercial ambitions. Isomorphic Labs, a DeepMind spinoff company in London, is applying AlphaFold3 to drug discovery.
But the publication of AlphaFold3 without its code or model weights — parameters obtained by training the software on protein structures and other data — drew criticism from scientists, who said the move undermined reproducibility. DeepMind swiftly reversed course and said it would make an open-source version of the tool available within half a year.
Anyone can now download the AlphaFold3 software code and use it non-commercially. But for now, only scientists with an academic affiliation can access the training weights on request.
DeepMind has got competition: over the past few months, several companies have unveiled open-source protein structure prediction tools based on AlphaFold3, relying on specifications described in the original paper known as pseudocode.
Two Chinese companies — technology giant Baidu and TikTok developer ByteDance — have rolled out their own AlphaFold3 inspired models, as has a start-up in San Francisco, California, called Chai Discovery.

AlphaFold3 — why did Nature publish it without its code?
A key limitation of these models is that, like AlphaFold3, none is licensed for commercial applications such as drug discovery, says Mohammed AlQuraishi, a computational biologist at Columbia University in New York City. However, Chai Discovery’s model, Chai-1, can be used via a web server for such work, says Jack Dent, a co-founder of the company.
Another firm, San Francisco-based Ligo Biosciences, has released a restriction-free version of AlphaFold3. But it doesn’t yet have the full suite of capabilities, including the capacity to model drugs and molecules other than proteins.
Other teams are working on versions of AlphaFold3 that don’t come with such limits: AlQuraishi hopes to have a fully open-source model called OpenFold3 available by the end of the year. This would enable drug companies to retrain their own versions of the model using proprietary data, such as the structures of proteins bound to different drugs, potentially improving performance.
The last year has seen a flood of new biological AI models released by companies with varying approaches to openness. Anthony Gitter, a computational biologist at the University of Wisconsin-Madison, has no problem with for-profit companies joining his field — so long as they play by the same rules as other scientists when they share their work in journals and preprint servers.
If DeepMind makes claims about AlphaFold3 in a scientific publication, “I and others expect them to also share information about how predictions were made and put the AI models and code out in a way that we can inspect,” Gitter adds. “My group’s not going to build on and use the tools that we can’t inspect.”

Not all ‘open source’ AI models are actually open: here’s a ranking
The fact that several AlphaFold3 replications have already emerged shows that model was reproducible, even without open-source code, says Pushmeet Kohli, DeepMind’s head of AI for science. He adds that in future he would like to see more discussion about the publishing norms in a field increasingly populated by both academic and corporate researchers.
The open-source nature of AlphaFold2 led to a flood of innovation from other scientists. For instance, the winners of a recent protein design contest used the AI tool to design new proteins capable of binding a cancer target. Jumper’s favourite recent AlphaFold2 hack was from a team that used the tool to identify a key protein that helps sperm attach to egg cells.
Jumper can’t wait for such surprises to emerge after sharing AlphaFold3 — even if they don’t always bear fruit. “People will use it in weird ways,” he predicts. “Sometimes it will fail and sometimes it will succeed.”
[ad_2]
Source link

[ad_1]
Welcome to the healthier, happier world of 2030. Heart attacks and strokes are down 20%. A drop in food consumption has left more money in people’s wallets. Lighter passengers are saving airlines 100 million litres of fuel each year. And billions of people are enjoying a better quality of life, with improvements to their mental and physical health.
These are just some of the ways in which analysts forecast that the new wave of incredibly effective weight-loss drugs, known as GLP-1 agonists, might transform societies and save countries trillions of dollars in the long run. The best known is semaglutide, marketed as Ozempic for diabetes, and as Wegovy for weight loss. “Short of some crazy unfortunate side effect, this is going to change the world,” says Chin Hur, a gastroenterologist at Columbia University in New York City.
It might have already started. In the United States, where 12% of adults say that they have at some stage taken GLP-1 agonists for diabetes or weight loss (see ‘Uptake of GLP-1 drugs in the United States’), media reports suggest that obesity rates are falling, although scientists caution that the data are not statistically significant (see ‘US obesity rates’). Slowing or reversing obesity trends more widely — more than half of the world’s population is expected to be overweight or have obesity by 2035 — would have myriad ripple effects. “The spillover impacts of obesity are enormous,” says Alison Sexton Ward, an economist at the University of Southern California in Los Angeles.

Source: KFF & US NCHS/CDC
But although scientists agree that the drugs could have huge impacts, there is a lot of uncertainty. Efforts to model the weight-loss drugs’ future impact are highly speculative for various reasons, ranging from their high costs to their long-term biological effects, and the big unknown of how people’s behaviour will change. All that has medical researchers and companies scrambling to gather more data and develop better tools to assess how weight-loss drugs might transform societies.

Source: KFF & US NCHS/CDC
Modelling obesity — and its prevention — has long been a staple of public-health research. One way of doing so is to create algorithms that simulate interventions, such as a tax on sugary drinks, or mandatory exercise programmes in schools. By shifting variables such as people’s willingness to cooperate or societal demographics, such models can estimate the health problems that would be prevented or the money that would be saved.
Such policy-based behavioural interventions usually have little effect on preventing weight gain or causing weight loss in the real world, at least in the short term. But the GLP-1 drugs could be different, says Theo Vos, an epidemiologist at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington in Seattle. Trials show that drugs such as semaglutide allow people to lose around 15% of their body weight in 16 months. Next-generation drugs could be even more effective. “This really works, and it works in quite a dramatic way,” says Vos.
The easiest things to model are the immediate impacts of a drug for an individual, including improvements both for physical ailments, such as reduced sleep apnoea, heartburn or joint pain, and in mental health, such as experiencing less social stigma. “If you lose weight, your quality of life improves immediately,” Hur says. Clinical trials suggest that the drugs seem to treat a host of other conditions, too, including addiction, Parkinson’s disease and infertility, but Hur says that it’s still too early to incorporate these benefits into models.

Why do obesity drugs seem to treat so many other ailments?
GLP-1 agonists do have downsides: many users experience nausea, gastrointestinal problems or muscle atrophy, and when people stop taking the drugs, they tend to quickly put the weight back on. Still, GLP-1s are probably different from previous ‘miracle’ weight-loss drugs such as fen–phen (fenfluramine/phentermine), which was banned because of its severe side effects, says Nicolas Rasmussen, a science historian at the University of New South Wales in Sydney, Australia. GLP-1s have been used to treat diabetes for many years and seem to be safe for most people.
Nevertheless, Rasmussen says, “history does tell us they’ll be overused”. Although the drugs might be clearly beneficial for people whose obesity is harming their health, people who take them simply to lose a few kilograms must set that benefit against the side effects. That hasn’t seemed to slow demand, especially as social-media influencers and celebrities promote the drugs for weight loss. Pharmaceutical companies that produce some of the key drugs have experienced shortages.
Beyond the effects on individuals, researchers expect that wide use of GLP-1 drugs could have some startling broader economic impacts. Analysts project that a global market already worth US$47 billion this year will grow ten-fold by 2032. People in certain industries, such as the food sector, are already becoming worried by the popularity of the drugs. An analysis by US investment firm Morgan Stanley predicted that US calorie consumption could drop by 1.3% by 2035. Last October, John Furner, the chief executive of retail company Walmart U.S., said that the company had seen a drop in food sales that it attributed to weight-loss drugs. Some analysts have projected less-obvious effects. US investment firm Jefferies predicted for one US airline that, if every passenger flying with it lost roughly 10 pounds (4.5 kilograms), the airline would save more than 100 million litres of fuel per year. Other reports found potential impacts for companies producing medical devices such as knee implants for arthritis or masks for sleep apnoea, more demand for smaller cars, and reconfiguration of land and building use if people walk more in commercial areas.
On a global scale, the ripple effects on economies could be even greater. For instance, studies suggest that young people with obesity perform worse in school1 and that girls are less likely to go on to pursue higher education than their non-obese counterparts are2, even when controlling for factors such as race, income and parents’ socioeconomic level or education. Obesity-related health problems have also been shown to lead workers to take more sick days — which in turn can lead to workplace discrimination.
Costs such as these account for more than 2% of global gross domestic product (GDP), according to a 2022 report on obesity rates in 161 countries3. If the rate of obesity increase was suddenly slowed by 5% relative to current trends, the report found, countries would save more than $429 billion each year between 2020 and 2060. Such analyses do not try to model the costs of drugs or any other intervention that could lead to lower obesity rates.
But when it comes to GLP-1 agonists, some of these predictions might be premature, says Ross Hammond, a systems scientist at the Brookings Institution, a think tank in Washington DC, because weight loss with GLP-1 agonists might not directly translate into global cost savings and health improvements. “I’d be very uncomfortable saying the cost estimates [in those studies] are costs that could be saved by everyone being on Ozempic,” he says. “It’s not clear all those consequences would be good.”
For instance, an economic principle known as moral hazard predicts that people tend to behave in risky or unhealthy ways if they face no consequence. It’s not yet clear whether people taking GLP-1 agonists adopt healthier lifestyles if they no longer have to worry about gaining weight, although some evidence suggests that the drugs reduce cravings for high-fat and high-sugar food. The same goes for exercise: research hasn’t yet shown whether people become more or less physically active if they lose weight with GLP-1 agonists.

Cheaper versions of blockbuster obesity drugs are being created in India and China
Hammond points out that exercise and healthy diets have benefits beyond weight maintenance. Reducing caloric intake alone won’t solve issues such as weak bones or muscles, driven by sedentary lifestyles and micronutrient deficiencies. “I’m a little worried that looking for a pharmaceutical solution will not address some of the bigger systems problems that we really face,” he says.
Vos agrees that modelling the health effects of weight loss with GLP-1 agonists isn’t straightforward. It’s unclear, he says, whether a drug that causes people to suddenly lose weight can be compared with an intervention that prevents them from gaining it in the first place. The duration of obesity might affect factors such as arthritis and cardiovascular risk, much as a person’s risk of lung cancer increases with the number of years that they smoked.
Michele Cecchini, a physician and economist at the Organisation for Economic Co-operation and Development (OECD) in Paris, says that there are other unknowns as well. For instance, many people regain weight years after undergoing bariatric surgery. That might turn out to also be the case for people who take weight-loss drugs for decades. “These are things that have a potentially huge impact at the population level,” he says.
Cecchini says that the OECD plans to release a report on GLP-1s’ economic impacts next year. His group has previously looked at the effects of obesity on factors such as education, workforce participation and health-care spending. Even climate change is affected when obesity rates rise. Carbon dioxide levels from food manufacturing rise to meet increased demand — particularly with red-meat production — and vehicles have greater emissions owing to heavier loads4.
The challenge with weight-loss drugs, Cecchini says, is the lack of long-term data. There’s a particular lack of independent studies, because many are funded by the drugs’ manufacturers, he adds.
Some data are more solid than others. Researchers could probably confidently project the drug’s impact in people in their sixties and seventies with high body mass indexes (BMIs), says Zachary Ward, a decision-science researcher at the Harvard T.H. Chan School of Public Health in Boston, Massachusetts. The effects of obesity on conditions such as diabetes, Alzheimer’s disease and certain cancers that affect this age group are well known.
A study of more than 17,000 people that was published last November5 estimated that Wegovy reduced the risk of heart attacks and strokes by 20% in people who had cardiovascular disease and were also overweight. And another research team estimated that 93 million people in the United States could benefit from Wegovy. If these people all took Wegovy, the team calculated, it would prevent 1.5 million cardiac events over ten years6.
But young people taking GLP-1 agonists are unlikely to encounter these diseases for many years, and factors such as lifestyles and environmental exposures can change over decades. “The longer you go, the more assumptions you make,” Ward says.
Some models show that younger people might benefit most from GLP-1 agonists — if they take them for the rest of their lives. Sexton Ward’s group found that, contrary to conventional wisdom, the drugs are less cost-effective for people with very high BMIs7. Rather, they can prevent more diseases in young people with BMIs between 30 and 40 — the lower end of the range for obesity. “That’s the range where it’s effective enough that 20% weight reduction will reduce the risk of comorbidities,” she says.

Obesity drugs aren’t always forever. What happens when you quit?
Their analysis found that, if everyone in the United States had free access to semaglutide, the resulting drop in obesity-associated diseases would save taxpayers $24.5 billion per year, although this would not include the cost of the drugs themselves.
Sexton Ward agrees that predicting population-level health and economic impacts is difficult owing to scarce data. But she highlights one idea: in a report funded by semaglutide-maker Novo Nordisk that she co-authored, her team found that the GLP-1s could produce much greater economic benefits for Black and Hispanic people in the United States than for white populations8.
US Black and Hispanic populations are, on average, more prone to obesity and related conditions than white populations are — largely because of societal inequalities such as lower average incomes and concomitant difficulties in accessing healthy food. Obesity, in turn, exacerbates other health disparities caused by environmental exposures and discrimination in health care.
“Over time, access to these drugs could begin to shrink some of these disparities,” Sexton Ward says. Although obesity isn’t the only cause of health inequality, she says, “I think it could be a step in the right direction.”
Right now, however, the drugs are so expensive that only relatively wealthy people can afford them (although in some US states, there is government health-care coverage under a programme for low-income individuals). If influencers and celebrities can easily lose weight, Rasmussen says, the stigma against obesity might increase. That could further harm people on low incomes, who are most likely to face the social, economic and health consequences of obesity. “That gap will increase as long as it remains expensive,” he says.
The high cost is a particular problem for low- and middle-income countries, where obesity rates are growing twice as fast as in high-income nations, says Adeyemi Okunogbe, a health-policy researcher at the non-profit RAND Corporation in Santa Monica, California. Of the estimated 5 million deaths each year caused by obesity-associated conditions, 77% occur in low- and middle-income countries.
Okunogbe says that obesity-related health-care costs put a double burden of disease on these countries, many of which are already fighting higher rates of infectious diseases. Other costs, such as lost wages owing to higher rates of illness and disabilities, are also magnified in lower-income nations. And in countries without national health systems, individuals would need to pay for GLP-1 agonists out of their own pocket. “It’s a long way off to consider this medicine in this context,” Okunogbe says.
Even countries with public health-care systems are struggling to work out how to pay for the drugs. The UK National Health Service currently funds semaglutide for individual weight loss for only two years, even though the drug must be taken for life to sustain its effect. And US law doesn’t require taxpayer-funded insurance programmes to cover weight-loss treatments (although the same drugs can be covered to treat diabetes). The drugs aren’t even close to affordable: an analysis last year9 by Hur’s group found that the cost of semaglutide would need to drop by 85% to make it cost-effective for adolescents. “The way things stand, there’s not going to be much impact on global health outcomes,” Ward says.
Cecchini says that the OECD’s analysis will consider the impact of cheaper generic and compounded GLP-1 agonist drugs, which are beginning to appear on the market in many countries. And some lawmakers, including in the United States, are beginning to push back on the high costs, particularly after an analysis found that Novo Nordisk could sell Ozempic for $5 per month and still make a profit10.
Until more people can afford the drugs, economists and public-health researchers hoping to look at global impacts are stuck with virtual models instead of studies of actual behaviour. “These drugs hold so much promise, but [the world] has to have access to realize it,” Sexton Ward says.
[ad_2]
Source link

[ad_1]
Organic molecules, which contain carbon (pictured), form certain shapes because of how their atoms bond.Credit: Dennis Kunkel Microscopy/Science Photo Library
For the first time, chemists have made a class of molecules previously thought too unstable to exist, and used them to generate exotic compounds1. Scientists say these notorious molecules, known as anti-Bredt olefins (ABOs), offer a new path to synthesizing challenging drug candidates.
The work is “a landmark contribution”, says Craig Williams, a chemist at the University of Queensland in Brisbane, Australia. The findings are published in Science.
Organic molecules, which contain carbon, typically conform to specific shapes because of the way their atoms bond together. For instance, olefins, also called alkenes — hydrocarbons that are often used in reactions for drug development — have one or more double bonds between two carbon atoms, resulting in the atoms being arranged in one plane.
The 100-year-old Bredt’s rule — which was proposed in 1924 by organic chemist Julius Bredt — states that, in small molecules made up of two rings that share atoms, such as some types of alkene, double bonds between two carbon atoms cannot occur where the rings join together, called the bridgehead position. This is because the bonds would force the molecule into a tortured, strained 3-D shape that makes it highly reactive and unstable, says study co-author Neil Garg, a chemist at the University of California, Los Angeles. “Still, 100 years later, people would say these types of structures are forbidden or too unstable to make,” he says.
Although the rule has made its way into chemistry textbooks, it hasn’t stopped researchers from trying to break it. Previous research has hinted that it’s possible to create ABOs that have a double carbon–carbon bond at the bridgehead position2. But attempts to synthesize them in their complete form were unsuccessful because the reaction conditions were too harsh, says Garg.
In the latest attempt, Garg and his colleagues treated a precursor compound with a fluoride source to kick-start a milder ‘elimination’ reaction, which removes groups of atoms from molecules. This resulted in a molecule that had the telltale ABO double-carbon bond. When the researchers added various trapping agents — chemicals that capture unstable molecules as they react — to this 3D ABO, they were able to produce several complex compounds that could be isolated. This suggests that the reactions of ABOs with different trapping agents can be leveraged to synthesize 3D molecules, which are useful for designing new drugs, says Garg.
Unlike typical alkenes, ABOs are chiral compounds — molecules that don’t perfectly match up with their mirror image. Garg and his colleagues synthesised and trapped an ABO that was enantioenriched, which means they produced more of one mirroring pair than the other. This finding suggests that ABOs could be used as unconventional building blocks for enantioenriched compounds, which are widely used in pharmaceuticals.
Chuang-Chuang Li, a chemist at the Southern University of Science and Technology in Shenzhen, China, says that the approach could be used to explore innovative synthesis pathways for other challenging molecules, such as the chemotherapy drug paclitexal (sold as Taxol) — a complex, multi-ringed molecule that is difficult to create in the laboratory. “It’s a valuable and reliable method,” says Li.
Garg and his team are exploring other reactions involving ABOs, and are investigating how to synthesize other molecules with seemingly impossible structures. “We can be thinking a little bit more outside of the box,” he says.
[ad_2]
Source link

[ad_1]

Brain activity is shown in gold (artist’s illustration). A newly approved antipsychotic achieves its effects by activating brain proteins called muscarinic receptors.Credit: Sebastian Kaulitzki/Science Photo Library
The first schizophrenia medication in decades with a new mechanism of action won US regulatory approval today. The approval offers the hope of an antipsychotic that would be more effective and better tolerated than current therapies.
The drug, known as KarXT, targets proteins in the brain known as muscarinic receptors, which relay neurotransmitter signals between neurons and other cells. Activating these receptors dampens the release of the chemical dopamine, a nervous-system messenger that is central to the hallmark symptoms of schizophrenia, such as hallucinations and delusions.
Pruning hypothesis comes of age
But muscarinic signalling also modulates other brain circuits involved in cognition and emotional processing. This mode of action provides KarXT with a more comprehensive therapeutic effect than other schizophrenia treatments, which mainly blunt dopamine activity alone.
In clinical trials, KarXT not only alleviated core symptoms of schizophrenia, but also showed signs of improving cognitive function, all while avoiding many of the burdensome side effects commonly associated with older antipsychotics.
“This will be a revolution of the treatment of psychosis, and I’m not saying this lightly,” says Christoph Correll, a psychiatrist at the Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York, who helped to analyse data from the trials. “Now we will now be able to treat people who haven’t been helped with traditional antipsychotics. That’s highly exciting.”
KarXT is just the first of many next-generation drug candidates designed to engage muscarinic receptors in the brain. Several follow-on schizophrenia therapies are already in or nearing clinical trials, showing promise for improved tolerability and more convenient dosing schedules.
This progress is leading clinicians and drug developers to imagine a future in which schizophrenia treatment becomes more tailored to individual needs — providing an alternative for the many people who don’t benefit from current therapies or abandon them owing to intolerable side effects.
“This provides an option that is completely outside the toolbox that we have right now,” says Ann Shinn, a psychiatrist at McLean Hospital in Belmont, Massachusetts, who has no commercial ties to KarXT.
KarXT traces its roots back to early 1990s, when researchers at Eli Lilly in Indianapolis, Indiana, began developing xanomeline — a muscarinic-activating agent designed mainly to boost memory in people with Alzheimer’s disease, but it has been explored as a potential treatment for schizophrenia, too.
Trials showed that the drug offered both antipsychotic and cognitive benefits1,2. But xanomeline also caused nausea, vomiting and stomach pain — because muscarinic receptors are active in the gut as well as the brain — leading Lilly to ultimately shelve the drug.

Flashes of activity (red and yellow; artificially coloured) light up the brain of a person having hallucinations caused by schizophrenia.Credit: Wellcome Centre Human Neuroimaging/Science Photo Library
Years later, biotech executive Andrew Miller devised a strategy to revive the therapy. He recognized that administering the muscarinic-activating agent together with another compound that blocks xanomeline’s effects outside the brain could maintain the cognitive and antipsychotic benefits without causing severe gastrointestinal distress.
In 2009, Miller formed a company called Karuna Therapeutics, based in Boston, Massachusetts. Karuna combined xanomeline with a drug called trospium. This well-understood molecule blocks muscarinic receptors and does not cross the blood–brain barrier, meaning that it selectively prevents side effects in the gut without interfering with xanomeline’s action in the brain.
Thus KarXT was born.
In clinical trials, the two-in-one pill outperformed a placebo in relieving characteristic symptoms of schizophrenia3,4, without the weight gain, sedation or movement issues that are commonly associated with existing antipsychotics. The side effects of KarXT were largely limited to gut disturbances, which tended to resolve after a week or two of daily use.
There were also strong signs of cognitive benefit, with preliminary indications5 that KarXT might also help to mitigate symptoms such as blunted affect and lack of motivation. “It’s encouraging,” Stephen Marder, a psychiatrist at the University of California, Los Angeles, says of these ancillary effects. (Marder assisted with some of the analyses). But these effects need to be verified in a “focused study,” he says.
The drug has a few shortcomings. For one, it requires twice-daily administration, and studies indicate that more frequent dosing schedules are linked to higher rates of non-adherence and treatment discontinuation in people with schizophrenia6. “That’s a big limitation,” says Nate Sutera, a psychiatric pharmacist at the University of Nebraska Medical Center in Omaha — particularly because many antipsychotics are now available as long-acting injectables, requiring only a few doses annually.
KarXT also comes with an anticipated price tag of roughly US$20,000 per year7, raising concerns among health economists about its cost-effectiveness compared with alternatives. Despite this, most industry analysts predict strong demand, with peak annual sales projected in the billions. This potential drove Bristol Myers Squibb (BMS) in Princeton, New Jersey, to acquire Karuna for approximately $14 billion this year.

First genomic study of schizophrenia in African people turns up broken genes
Other drug makers are likewise seeing the value of targeting muscarinic receptors, pursuing various strategies to improve on the profile of KarXT. Some are developing formulations with more convenient dosing schedules. Others are focused on greater target selectivity, aiming to design molecules that activate only specific muscarinic receptors — either the M1 receptor, linked to cognitive benefits, or the M4 receptor, which underpins antipsychotic effects, but not both, as KarXT does.
One such drug candidate, an M4-selective agent called emraclidine, seems to offer antipsychotic effects similar to those of KarXT, with improved tolerability, although it offers potentially fewer cognitive benefits, according to early clinical testing8.
Former Karuna chief executive Steven Paul, a psychiatrist now at the Washington University School of Medicine in St. Louis, Missouri, welcomes the wave of innovation in targeting muscarinic signalling that KarXT helped to unleash — and he looks forward to discovering the best ways to harness this therapeutic strategy.
“Now we have new biology and new pharmacology to explore,” he says. “It will be fun and scientifically relevant — and, hopefully, clinically beneficial to patients — to find out.”
[ad_2]
Source link

[ad_1]
In 2022, more than 80,000 people died of an opioid overdose in the United States. To reduce this toll, we need to abandon analgesic drugs that act through the µ-opioid receptor and identify painkillers that cannot be so easily abused. Fortunately, developments in how we can evaluate the efficacy and adverse effects of drugs are making this possible.
In 1985, the World Health Organization (WHO) proposed an ‘analgesic ladder’ to provide pain relief for people with cancer, it recommended non-steroidal anti-inflammatory drugs (NSAIDs) for mild pain; a combination of an NSAID and a weak opioid for moderate pain; and strong opioids for severe pain1. Although well-intentioned, this framework unfortunately promoted the use of opioids by providing access to these addictive substances.
Nature Outlook: Pain
There were three fundamental flaws to the WHO strategy. The first was the assumption that the severity of pain is the only important factor to consider when selecting a suitable treatment. The second was the presumption that µ-opioid receptor agonists would be effective for all types of severe acute or chronic pain. And the third problem was the expectation that prescription opioids could be distributed safely.
After almost four decades, the WHO ladder remains widely used by clinicians — even though we now appreciate that opioids are highly dangerous. Scientists also recognize that there are several distinct types of pain, each driven by different mechanisms and requiring specific distinct interventions. These include nociceptive pain, which is initiated by tissue damaging stimuli; inflammatory pain that is associated with the activation and recruitment of immune cells; neuropathic pain owing to damage to the nervous system; and nociplastic pain, which reflects pathological dysfunction of the nervous system.
Researchers have now identified sensory neurons in the peripheral nervous system that trigger pain. They have also discovered immune drivers of pain2, as well as the specific circuits in the central nervous system that generate the sensation of pain and the modulatory circuits that suppress pain3. Scientists have also worked out how these circuits can change to drive persistent clinical pain, which is pathological and quite distinct from the protective aspects of acute nociceptive pain that warns of danger in the environment. We now have sufficient understanding of pain mechanisms to identify analgesic drugs that can reduce pathological pain without eliminating the protective function of acute physiological pain.
With these pieces in place, the key question becomes: what is the best way to set up an effective and efficient analgesic discovery platform that will identify the sort of drugs that are so urgently needed?
The standard industry approach is to identify a single target that might contribute to a disease state; validate it by conducting gain- and loss-of-function manipulations in animal models and in vitro assays, and by using human genetics; and then run screens for compounds that act only on the target. (A target can be a receptor, ion channel or enzyme.) Unfortunately, this has not worked well; there have been few approvals of analgesics acting on new targets over the past decade. One reason for this is that compounds that act on multiple targets might be required.
Clearly, an alternative strategy is needed. One option with great promise is a technique called phenotypic screening, which identifies drugs with cell-selective or disease-modifying activity. This method can detect a particular observable characteristic of a cell, such as its excitability. This is possible because human induced pluripotent stem cells can be differentiated into any cell type and used in diverse ways to model and measure disease states.
Scientists can generate human nociceptors — the sensory neurons that trigger pain in response to noxious stimuli — to study pain in a dish4. In unpublished work, researchers have been able to screen for compounds that selectively reduce activity only in these neurons without affecting other excitable cells, thereby silencing peripheral pain triggers. Furthermore, researchers can run phenotypic screens to identify analgesics that reduce the heightened sensitivity of nociceptors. An important element of these phenotypic screens is that, because they use human cells, there is no risk of wasting development resources on compounds that won’t work in people.
More from Nature Outlooks
In conventional drug discovery for medicinal chemistry, compound profiles (or hits) are designed on the basis of the interaction between the compound and the active side of the target protein. By contrast, phenotypic screens will need to be developed using different methods because of the lack of a single target in which the structure and interaction with drugs can be directly determined. Among the most promising technologies is artificial-intelligence-tool-based drug design.
Machine learning is also assisting efforts to identify analgesics by helping to assess behaviour in rodents, enabling identification of reliable surrogates both of clinical pain states and adverse effects, as well as identifying drugs that are likely to be misused5.
This strategy will provide us with the means to identify effective and safe analgesics, and in turn permit us to at last abandon prescription opioids.
The author declares no competing interests.
[ad_2]
Source link

[ad_1]
There’s a bar in Baltimore, Maryland, that very few people get to enter. It has a cocktail station, beer taps and shelves stacked with spirits. But only scientists or drug-trial volunteers ever visit, because this bar is actually a research laboratory. Here, in a small room at the US National Institutes of Health (NIH), scientists are harnessing the taproom ambience to study whether blockbuster anti-obesity drugs might also curb alcohol cravings.
Evidence is mounting that they could. Animal studies and analyses of electronic health records suggest that the latest wave of weight-loss drugs — known as glucagon-like peptide 1 (GLP-1) receptor agonists — cut many kinds of craving or addiction, from alcohol to tobacco use.
“We need randomized clinical trials as the next step,” says Lorenzo Leggio, an addiction researcher at the NIH in Baltimore. In the trial he is leading, volunteers sit at the bar and get to see, smell and hold their favourite drinks, while going through tests such as questions about their cravings; separately, participants will have their brains scanned while looking at pictures of alcohol. Some will be given the weight-loss drug semaglutide (marketed as Wegovy) and others will get a placebo.

Addiction researcher Lorenzo Leggio (right) with colleague George Koob in the research laboratory bar at the US National Institutes of Health.Credit: Cliff Owen/AP/Alamy
Curbing addiction isn’t the only potential extra benefit of GLP-1 drugs. Other studies have suggested they can reduce the risk of death, strokes and heart attacks for people with cardiovascular disease1 or chronic kidney ailments2, ease sleep apnoea symptoms3 and even slow the development of Parkinson’s disease4. There are now hundreds of clinical trials testing the drugs for these conditions and others as varied as fatty liver disease, Alzheimer’s disease, cognitive dysfunction and HIV complications (see ‘Diseases that obesity drugs might treat’ at the end of this article).
“We’re in a phase where GLP-1-based drugs are being considered as potential cures for every condition under the Sun,” says Randy Seeley, an obesity specialist at the University of Michigan in Ann Arbor, who has consulted for and received research funding from several firms that develop obesity drugs.

How rival weight-loss drugs fare at treating obesity, diabetes and more
It could take years to prove in which cases the drugs are useful. Understanding how they work could be even harder. In some instances, such as for people with cardiovascular disease, the reason seems straightforward: weight loss is almost certainly providing much of the benefit. But the effects observed in conditions such as addiction and Parkinson’s disease involve other mechanisms that are far from being unravelled.
Working them out, Leggio notes, could help to explain why some people respond better than others to the drugs, and how to mitigate potential side effects, such as nausea, constipation, a reduction in muscle mass during weight loss, and (in rare cases) pancreatitis.
Drugs that work and are safe might be enough for most clinicians and people seeking treatment, says Daniel Drucker, an endocrinologist at the University of Toronto in Canada who consults for and receives research funding from obesity-drug firms. “But if you are trying to capitalize on a possible therapeutic effect and make the next generation of a drug even better, then you ought to know where it is working and how it is working,” he says.
The key property of obesity drugs is that they mimic the natural GLP-1 hormone and activate the same receptors that it would typically target. But because the synthetic drugs are long-lived, their effects extend well beyond those of the hormone they copy5.
There are two natural GLP-1 systems in the body: one in the gut and one in the brain. After each meal, cells in the lining of the intestine produce GLP-1. This stimulates the pancreas to release insulin, which helps to regulate blood-sugar levels, suppress appetite and slow down digestion.
The second system activates only under specific conditions, such as after a large meal or in response to a stressor such as an infection. In these instances, neurons in the hindbrain — the lower back region of the brain, including part of the brainstem — can also produce GLP-1, and there are receptors for the hormone in many neurons across the brain. They include those involved in appetite control, mood regulation, reward and movement.
These systems seem to be entirely separate. It was once thought that gut GLP-1 communicates with the hindbrain neurons by signalling through the vagus nerve (which goes up through the brainstem), but researchers have shown that these systems don’t typically interact6. The gut hormone is quickly metabolized after it is released into the bloodstream: it disappears in only a few minutes.
Synthetic GLP-1 drugs, by contrast, last much longer in the body — a week or more in the case of semaglutide and another drug called tirzepatide. That gives them a better chance of getting into the brain (see ‘Where do obesity drugs act?’).

It’s likely that the drugs are targeting GLP-1 receptors both in peripheral organs and in the brain, says Karolina Skibicka, a neuroscientist at Penn State University in University Park, Pennsylvania, and at the University of Gothenburg, Sweden, who has also received funding from and consulted for obesity-drug firms. “That’s a big difference from what our physiology normally does,” she says. “This is part of the reason why these drugs have been so successful in not only treating obesity, but potentially other conditions,” she adds.
It remains unclear how deep into the brain the drugs actually get. Animal studies suggest that some drugs in this class can cross the blood–brain barrier, the protective layer that dictates which substances can move into the brain7. But some scientists say the drugs can’t penetrate deeply and are only able to access certain regions where the blood–brain barrier might be leaky, potentially setting off a cascade of signals from there. (An industry-sponsored study found that semaglutide does not cross the blood–brain barrier8.)
“These drugs are able to activate regions deep within the brain that they clearly can’t penetrate. And this is still a mystery,” says Drucker, whose research on the hormone GLP-1 contributed to the development of the drugs.
Despite that mystery, it’s becoming clear that obesity drugs might suppress addiction in ways related to how they suppress appetite.
For appetite control, animal studies suggest that the drugs act predominantly on GLP-1 receptors on neurons located in the hypothalamus and the hindbrain. These regions regulate functions such as hunger, body temperature and heart rate.

Obesity drugs aren’t always forever. What happens when you quit?
But that’s not all they do. The drugs also affect neural pathways that govern taste, reward and value — a property that neuroscientists call salience, says Allison Shapiro, a specialist in neurodevelopment at the University of Colorado Anschutz Medical Campus in Aurora. The neurotransmitter dopamine has an important role in these pathways, but it’s not the only player: the circuits are complex and not fully understood.
The drugs’ effects on reward and salience suggest why they might also affect cravings and addiction, says Leggio. They are thought to dampen the brain’s reward system so that an individual might not feel the urge to drink another glass of wine, smoke another cigarette or eat another slice of pizza to get that extra rush of pleasure. This doesn’t necessarily mean that the drugs would reduce people’s ability to feel pleasure, only that they might be less inclined to repeat their behaviours in a continuous search for reward.
There is another factor to consider in the case of addiction, Leggio adds: substances such as alcohol and methamphetamine can disrupt the blood–brain barrier, potentially affecting the action of GLP-1 drugs. “Giving a drug of this kind to someone who is a healthy person may be different from giving the same medication to someone who has an addictive disorder and whose blood–brain barrier has been destroyed,” he says.
GLP-1 medications are being tested as ways to treat multiple substance-use disorders. One small trial — unpublished, but presented at a conference in February — found that people undergoing treatment for opioid-use disorder who took a GLP-1 drug called liraglutide reported a 40% reduction in opioid cravings. Another study is evaluating the potential of exenatide, another GLP-1 mimic, to treat cocaine addiction. Clinical trials are also investigating whether semaglutide, liraglutide and exenatide can help people to stop smoking.

A number of obesity drugs are being trialled for their ability to cut nicotine cravings.Credit: Jakub Porzycki/NurPhoto via Getty
For some conditions, the benefits of these drugs stem directly from weight loss. People with cardiovascular disease, for instance, are known to benefit from losing weight and consequently shedding accumulated fat that might contribute to clogged arteries. Unsurprisingly, a trial found that people with heart disease who were obese or overweight reduced their risk of having a severe cardiovascular event — including death, stroke or heart attack — by 20% when they took semaglutide1.
Weight loss is also an effective therapy for people with obstructive sleep apnoea, because excessive weight leads to fat deposits in the neck, which can temporarily block airways during sleep. A trial of tirzepatide showed benefits for this condition3.

Cheaper versions of blockbuster obesity drugs are being created in India and China
Perhaps less obviously, weight loss also explains why semaglutide eases a condition that affects the ovaries, called polycystic ovary syndrome (PCOS). Studies had already established that losing weight and following a healthy diet can help to reduce the symptoms of PCOS, which is associated with excess testosterone, irregular or missed periods and insulin resistance, a condition in which the body’s cells have trouble using insulin to absorb sugar (glucose) from the blood.
In a clinical trial presented last year (but not yet published in a journal), researchers treated girls and young women with PCOS who were obese with either semaglutide or an intensive dietician-led programme over four months. Both groups experienced reductions in testosterone and an increased number of periods. In the semaglutide group, the more weight participants lost, the greater their improvements9. “What we found was that semaglutide, as expected, improves glucose metabolism. But all the other reproductive and metabolic improvements were because of the weight loss,” says Melanie Cree, a paediatric endocrinologist at the University of Colorado Anschutz Medical Campus who led the trial.
But there are plenty of conditions in which weight loss doesn’t explain the drugs’ benefits. One clinical trial in people with type 2 diabetes and chronic kidney disease found that semaglutide cut the risk of serious kidney complications — including the need for dialysis and transplantation — by 24%. The study2 concluded that the mechanism of kidney protection was unrelated to changes in the participants’ body weight. The authors hypothesize, instead, that the drug acts by reducing inflammation in the kidney.

Semaglutide, marketed as Wegovy, reduced serious kidney complications in a trial in people with type 2 diabetes.Credit: M. Scott Brauer/New York Times/Redux/eyevine
Inflammation occurs when immune cells rush to the site of an injury or illness to start the healing process. But if it becomes chronic, this can contribute to health problems. Animal experiments have demonstrated that drugs that act on GLP-1 receptors can dampen inflammation in the kidneys, heart and liver.
That helps to explain the positive effects of survodutide — a drug that mimics both GLP-1 and glucagon, another hormone involved in blood-sugar regulation — in a type of fatty liver disease called metabolic dysfunction-associated steatohepatitis. In a clinical trial, the drug led to improvements in the condition in 47–62% of participants, depending on the dose they received10.
The mechanism involves the brain as well as the peripheral organs. There are plenty of places in the body where GLP-1 receptors can be found on immune cells, so that’s one obvious route. But in some tissues where the drugs reduce inflammation, there aren’t many GLP-1 receptors around. A study last year found that in such organs, GLP-1 receptors in the brain are likely to be responsible for the anti-inflammatory effects. When researchers blocked GLP-1 receptors in animals’ brains using genetic methods or drugs, the treatments no longer reduced inflammation in multiple tissues, confirming the connection11.
The anti-inflammatory effect might also explain how GLP-1 drugs help to ease the symptoms of neurodegenerative diseases such as Parkinson’s4,11 and Alzheimer’s disease. Approved drugs for the conditions don’t target the excessive brain inflammation that is characteristic of these diseases.
In one trial, people with Parkinson’s who took exenatide had significantly improved motor abilities compared to people who received a placebo12. A larger, phase III clinical trial testing the same drug is currently under way, with results expected this year. Tom Foltynie, a neurologist at University College London who is leading the work, started to explore the potential of exenatide in 2008, inspired by basic research demonstrating its neuroprotective properties in animal models.

How anti-obesity drugs cause nausea: finding offers hope for better drugs
Parkinson’s is partially caused by impairments in neurons’ mitochondria, the cellular organelles responsible for energy production. When cells run out of energy, they can’t repair themselves and cell connections stop working. This causes inflammation, which possibly further aggravates the situation, Foltynie says. Some of the affected neurons produce dopamine, which plays a part in movement and coordination and explains the major symptoms of the disease.
Foltynie’s hypothesis is that exenatide reduces inflammation and improves mitochondrial function, which might allow neurons to start working again, improving the motor symptoms.
Christian Hölscher, a neuroscientist at the Henan Academy of Innovations in Medical Science in Zhengzhou, China, says that the clinical evidence on the utility of GLP-1 drugs in Parkinson’s is already compelling and that, if positive, the phase III trial results for exenatide will be a game-changer for clinical practice. Hölscher is the chief scientific officer of Kariya Pharmaceuticals, a Danish biotech firm in Copenhagen that is exploring GLP-1 drugs as a way to treat neurodegenerative diseases.
He is now working on strategies to develop GLP-1 drugs that penetrate the brain in higher concentrations than for currently available drugs. “There’s a clear correlation between the ability to get into the brain and the neuroprotection effect,” he says.
A similar mechanism could explain some promising preliminary results for Alzheimer’s disease, too. Hölscher’s colleagues presented a small, unpublished study at a conference in July suggesting that cognitive decline in people with Alzheimer’s who took liraglutide was 18% slower over a year compared with those who were given a placebo.
Semaglutide is also being evaluated for treating early Alzheimer’s disease in two large clinical trials sponsored by the drug maker Novo Nordisk, based in Bagsvaerd, Denmark.
The list of potential uses for GLP-1 medications doesn’t end there. Because the drugs are thought to act on the neurotransmitter serotonin — the target of many antidepressants — researchers wonder whether they might have the potential to treat depression and anxiety.
For instance, Skibicka and her colleagues studied the effect of both the natural hormone GLP-1 and the drug exenatide in rats, and found that chronic administration of both substances reduced depression-like behaviour in these animals13.
Obesity drugs have another superpower: taming inflammation
It’s not clear whether the effects would be the same for humans, but at least one clinical trial is under way to evaluate semaglutide as a treatment for cognitive dysfunction — difficulties in thinking clearly, concentrating and memory — in people with major depressive disorder.
It’s increasingly hard to find a bodily system that isn’t touched in some way by the drugs. Researchers are also investigating how these drugs might affect fertility and exploring their potential to treat inflammatory conditions such as arthritis.
But the field should remain cautious, says Seeley — particularly when deciding whether people who aren’t overweight or obese should take the drugs, considering their side effects.
And Tamas Horvath, a neuroscientist at Yale University in New Haven, Connecticut, questions the portrayal of these medications as a cure-all — especially because researchers still don’t know what the long-term effects might be. “We don’t know the outcomes of using them continuously for years and decades,” he says.
[ad_2]
Source link

[ad_1]

Joel Habener (from left), Svetlana Mojsov and Lotte Bjerre Knudsen have won a 2024 Lasker Award for developing a class of drugs that treats obesity, diabetes and more.Credits: Joel Habener, Lori Chertoff for The Rockefeller University, Soren Svendsen
Three scientists involved in developing the blockbuster anti-obesity drugs that are currently changing the health-care landscape are among the winners of this year’s prestigious Lasker Awards. The prizes, which honour important advances in medical research, are often considered an indicator of whether a specific advance or scientist will win a Nobel Prize — and some are speculating that this could soon be the case for the weight-loss treatments.
The ‘breakthrough’ obesity drugs that have stunned researchers
Joel Habener, Svetlana Mojsov and Lotte Bjerre Knudsen each contributed to the creation of the popular anti-obesity drugs, which mimic a hormone called glucagon-like peptide 1 (GLP-1), involved in lowering blood-sugar levels and controlling appetite. The trio, recognized with a Lasker in the clinical-research category, will share a US$250,000 prize.
Biomedical scientists are enthusiastic about the increasing recognition of GLP-1 research, which was initially aimed at treating diabetes. “I’ve been working on this for 30 years, and for a long time nobody cared,” says Randy Seeley, an obesity specialist at the University of Michigan in Ann Arbor. “Over the last several years, the situation has changed so much. We now have therapies that are actually helping people.”
Other recipients of this year’s Lasker Awards include Zhijian ‘James’ Chen at UT Southwestern Medical Center in Dallas, Texas, who was honoured in the basic-research category for discovering how DNA triggers immune and inflammatory responses. In the public-service category, Salim Abdool Karim and Quarraisha Abdool Karim, both at the Centre for AIDS Programme of Research in South Africa, in Durban, were recognized for developing life-saving approaches to prevent and treat HIV infections.
Habener, an endocrinologist at Massachusetts General Hospital in Boston, was a leader in discovering the GLP-1 hormone in the 1980s. He was interested in understanding the hormones involved in type 2 diabetes, a condition characterized by high blood-sugar levels, in which the body either doesn’t produce enough insulin or has trouble using it to absorb sugar from the blood.
Habener zeroed in on glucagon, a hormone that increases blood-sugar levels. After cloning the gene for glucagon, he discovered that the gene also encoded a related hormone — later named GLP-1 — that stimulates the pancreas to produce insulin1.
Obesity drugs have another superpower: taming inflammation
“This was interesting because, rather than having to give injections of insulin to people with diabetes to control blood sugar, giving GLP-1 would theoretically prompt the body to make its own insulin,” Habener says.
Around that time, Mojsov, a biochemist who directed a facility producing synthetic proteins at Massachusetts General Hospital, identified the sequence of amino acids making up the biologically active form of GLP-1. Eventually, she would demonstrate that this active form could stimulate insulin release from a rat pancreas2 — a necessary step on the path to a human treatment.
Now at Rockefeller University in New York City, Mojsov spoke out last year about the lack of recognition for her contribution to the field. Since then, she has received awards such as the VinFuture Prize. “I’m happy that I’m getting awards, but what makes me even happier is that people are actually reading my work,” she says.

Ozempic keeps wowing: trial data show benefits for kidney disease
After the initial discoveries about GLP-1, researchers realized that there was a significant obstacle to its therapeutic use: the hormone was rapidly metabolized, lasting only a few minutes in the blood. That’s where the work of Knudsen, a scientist at pharmaceutical firm Novo Nordisk, in Copenhagen, came in. She and her team realized that regular GLP-1 was not going to work as a medicine, Knudsen says. Instead, the researchers came up with a way to modify GLP-1 by attaching a fatty acid to it — an alteration that allowed the molecule to remain active in the body for an extended period before degrading3.
The work resulted in liraglutide, the first long-lasting GLP-1-based drug, approved by the US Food and Drug Administration in 2010 for type 2 diabetes. In the meantime, researchers were already exploring the drugs’ weight-loss potential, and in 2014, liraglutide became the first molecule in its class to be approved for treating obesity. Today, newer variants, including semaglutide and tirzepatide, sold as Wegovy and Zepbound, are important obesity treatments.
“I really hope to inspire young people so that they can see that you can do great science also in the pharmaceutical industry,” Knudsen says.
GLP-1-based drugs don’t just treat obesity and diabetes. Studies have shown they can help with cardiovascular disease, sleep apnea and kidney disease, among other conditions. These benefits are thought to arise from the drugs’ effects on the brain, as well as their anti-inflammatory potential.

Meet the unsung scientists behind the Nobel for quantum dots
Owing to the shake-up these drugs are causing in health care, some think they might soon win science’s top prize — the Nobel. Winning a Lasker often precedes winning a Nobel prize: since 1945, 95 Lasker laureates have also received that top honour. “This raises the spectre that the Nobel committee will take [GLP-1 research] seriously,” Seeley says. The Nobel prizes will be announced next month.
Each prize in a science discipline is limited to no more than three winners, and the challenge will be to select the most deserving recipients. Several other scientists involved in the research behind GLP-1-based drugs have been recognized by other awards, including Jens Juul Holst at the University of Copenhagen, Daniel Drucker at the University of Toronto in Canada, and Richard DiMarchi at Indiana University in Bloomington.
“It’s 10,000 ants that move the anthill, and we’re trying to pick out the three ants that made the most difference,” Seeley says. “You could come up with a dozen names of people, at least, who have made seminal contributions to the field.”
[ad_2]
Source link