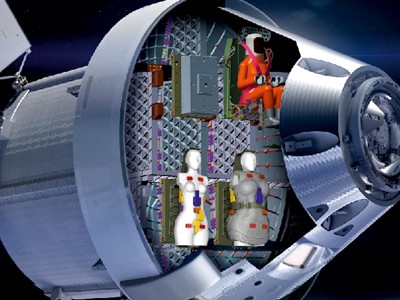
To understand the effects of radiation on the body, two female ‘phantoms’, Helga and Zohar, were strapped into the Orion capsule as part of the Artemis I mission and launched into space on November 16th 2022.
There is limited data on the effects of space radiation on the female body and, with future moon missions planned to have female crew, Helga and Zohar are key to filling that void. They were fitted with a multitude of detectors to determine the risks posed to future female astronauts.
Read the paper: Space radiation measurements during the Artemis I lunar mission
Space radiation comes in two forms, the ever present galactic cosmic rays and bursts of radiation from solar particle events. Both present different issues to the human body and, if humanity wants to pursue the idea of journeying to other planets, we need to understand our limits.
From repealing climate policies to overturning guidance on the safe development of artificial intelligence (AI), Republican Donald Trump made plenty of promises during his presidential campaign that could affect scientists and science policy. But fulfilling all of his pledges won’t be easy.
The US is the world’s science superpower — but for how long?
Trump, now the US president-elect for a second time, will have some advantages as he re-enters the White House in January. The first time he took office in 2017, his victory was a surprise, and many government watchers who spoke to Nature say that he didn’t have a solid plan. By contrast, the Trump administration that enters office next year will be better prepared, and Trump himself is likely to face fewer checks on his power now that he has consolidated control over the Republican establishment, says Matt Dallek, a political historian at George Washington University in Washington DC who studies the modern conservative movement.
But that still does not mean he will be able to do as he pleases, Dallek adds. “There’s a kind of revolutionary sweep to a lot of Trump’s promises that may collide with the messy reality of implementation.”
Here Nature talks to policy and other specialists about what might be in store on a range of science issues during a second Trump administration.
It will be possible for Trump to implement his plan as soon as he enters the White House given that executive orders can be revoked by a president at any time. But what will Trump put in its place?
‘We need to be ready for a new world’: scientists globally react to Trump election win
“The emphasis will shift away from the regulatory environment” and towards technology companies making their own voluntary decisions on safety, says Suresh Venkatasubramanian, director of the Center for Technological Responsibility, Reimagination, and Redesign at Brown University in Providence, Rhode Island. “I am personally sceptical that that will be enough” to address AI-associated risks to public safety, data-privacy concerns or the use of biased algorithms that disadvantage certain groups of people, Venkatasubramanian says.
Biden’s executive order emphasized making sure that AI models, which are trained on human-derived data, don’t output discriminatory results. That’s probably also not going to be a heavy priority for the new administration, Venkatasubramanian says. The Republican platform says that it will “support AI Development rooted in Free Speech and Human Flourishing”.
According to Roman Yampolskiy, a computer scientist and AI safety researcher at the University of Louisville in Kentucky, “it is a great idea to remove censorship and support free speech” in general. But, he says, “removing regulations around training of advanced AI systems is the worst possible thing we can do for the safety of the American people and the world”. Given the risks associated with developing superintelligent AI systems, which could potentially operate in unpredictable ways and cause harm to humans, Yampolskiy and other AI researchers have been arguing for a pause in AI development, which could only be achieved with stronger regulations.
Climate change
Many federal climate efforts are likely to stall or move in reverse under Trump, who has long denied the dangers of climate change while prioritizing the economic benefits of boosting domestic fossil-fuel production. Even so, policy specialists say that Trump is unlikely to stop the United States’s gradual shift towards clean energy.
The US election is monumental for science, say Nature readers — here’s why
For instance, it will not be easy to undo Biden’s signature climate achievement: the 2022 Inflation Reduction Act (IRA), which created a raft of federal investments now estimated at more than US$1 trillion in climate and clean energy that are scheduled to run until around 2032. Repealing that legislation would require an act of the US Congress. But even if Republicans end up in control of both congressional chambers, businesses and leaders in conservative US states that are already benefitting from IRA investments might not be eager to cut off the flow of federal money, says Joanna Lewis, who heads the science technology and international affairs programme at Georgetown University in Washington DC.
Trump could have a bigger — and more negative — impact on climate progress if he moves to weaken climate regulations put in place for things such as power plants and automobiles. Similarly, his promise to place new tariffs on goods from countries such as China and Mexico could actually increase the cost of clean-energy technologies, says David Victor, a political scientist at the University of California, San Diego.
The president-elect has also promised to once again pull the United States out of the 2015 Paris agreement, which commits member countries to limiting global warming to 1.5–2 °C above preindustrial levels. Trump’s administration had to wait until 2020 before formally leaving the agreement last time, and Biden moved to rejoin the agreement quickly after taking office several months later. But under the rules of the agreement, the leaving process would take only one year this time around.
Many climate observers say the absence of the United States — the world’s second-largest greenhouse-gas emitter — from the pact could reduce pressure on China and other nations to scale up their efforts to curb emissions just as time is running short. “This is a pivotal decade for climate action, and four more years of Trump could be disastrous in terms of mobilizing climate action,” Lewis says.
Health
In the weeks leading up to the US election, Trump teamed up with political figure Robert F. Kennedy Jr. on a platform promising to “make America healthy again” by tackling the root causes of chronic diseases, removing toxic substances from the environment and combatting corporate corruption. Trump has said that he will let Kennedy, who has questioned vaccine effectiveness, “go wild on” health, unnerving public-health and health-policy researchers.
It remains to be seen whether Trump will appoint Kennedy to a position such as director of US Health and Human Services (HHS) — or whether the US Senate would approve it — but it’s clear that Kennedy will have Trump’s ear on health issues.
Robert F. Kennedy Jr. ran for president in 2024 as an independent before withdrawing his bid and endorsing Trump.Credit: Rebecca Noble/Getty
Georges Benjamin, the executive director of the American Public Health Association in Washington DC, worries about Kennedy’s role in the new administration because he has long cast doubt on the vaccine-approval process, threatening to undermine confidence in jabs and cause a resurgence in illnesses such as measles. “People will get sick and die because of the confusion around vaccines, if [Kennedy and Trump] implement some of the things they verbalize,” he says.
Some of Kennedy’s goals, such as cracking down on ties to industry at regulatory agencies such as the US Food and Drug Administration, are noble, says Diana Zuckerman, president of the National Center for Health Research, a non-profit think tank in Washington DC. But those goals don’t jibe with what occurred during the first Trump administration, when Trump installed people with close industry ties to important health posts, such as former HHS director Alex Azar, so it’s hard to know what will happen, she says.
With Trump’s isolationalist approach and past comments he has made criticizing the World Health Organization, support for global health will also likely be “greatly scaled back” during Trump’s second term, says Ezekiel Emanuel, a bioethicist and long-time observer of the US biomedical funding landscape at the University of Pennsylvania in Philadelphia. The United States is “the key player” in funding of global-health initiatives, says Emanuel. This includes, for instance, a programme that aims to end the global AIDS epidemic. So it’s “hard to be optimistic” about the future, he adds.
Foreign science partnerships
During Trump’s first term, his administration barred people from a half-dozen countries that it said were “compromised by terrorism” from entering the United States and implemented an anti-espionage programme called the China Initiative that led to the arrests of scientists of Chinese heritage. The Biden administration overturned the travel ban and ended the China Initiative, but under Biden, federal officials have continued efforts to guard against foreign interference in US research.
US election debate: what Harris and Trump said about science
Specialists says it’s unclear whether the second Trump administration will revive the China Initiative, although the Republican-led US House of Representatives advanced legislation in September that would do so. But a reinstatement of the travel ban is likely, says Adam Cohen, a lawyer at Siskind Susser in Memphis, Tennessee, who focuses on academic immigration and who says the president has broad authority to institute such policies.
Like the first Trump administration, the new one will probably clamp down on granting visas to foreign researchers and students from some countries, says Jennifer Steele, an education policy researcher at American University in Washington DC. Policies that make it harder for international and US researchers to meet would also make it harder for new scientific collaborations to arise, says Caroline Wagner, a specialist in science, technology and international affairs at The Ohio State University in Columbus. That’s because such partnerships are fuelled by face-to-face contact. “Collaborations don’t begin with people just e-mailing each other across the miles,” she says.
But there might be one bright spot on the collaboration front, at least for US-China partnerships. Denis Simon, a non-resident fellow at the Quincy Institute for Responsible Statecraft, a foreign policy think tank in Washington DC, thinks that a crucial pact governing US-China scientific cooperation that has been expired for the past year is likely to be signed by the Biden administration before Trump’s second inauguration in January. A renewal of the agreement, although it is will probably be more limited in scope owing to increased US-China tensions, would show that “both governments give their blessing” to collaborations, Simon says.
California’s Inland Empire is a broad swath of land east of Los Angeles, about five times the size of Connecticut, stretching through desert and surrounded by mountains. It’s one of the state’s fastest-growing regions, but it’s underresourced, with incomes and education levels lower than the state average. It is also medically underserved, with too few primary care physicians and specialists to adequately tend to the area’s increasing population. In the region’s many Spanish-speaking communities, finding a doctor who speaks the same language is difficult. And whether people can communicate well with their health-care providers affects patient outcomes.
Three years ago the Inland Empire Free Clinic opened in Colton, Calif., to provide free health and medical care and social services. Its clinic is staffed by physicians and medical students from the nearby California University of Science and Medicine. Many are proficient in Spanish, and those who aren’t work through interpreters. “The moment I talk in Spanish to patients, they change their attitude and are more open to tell me how they actually feel,” says Alexandra Lopez Vera, director of C.U.S.M.’s medical Spanish program, who coordinates interpreters for the clinic. “If I talk to a Latina who comes to see a doctor because they have a problem related to the reproductive system, they may feel like, ‘I feel embarrassed to tell this white guy who doesn’t speak my language about this situation that I’m having.’ They request for me to be with them.”
Research has shown that in the U.S., patients with limited English proficiency have a higher risk of hospital readmission and greater difficulty adhering to medication regimens. More than 25 million people who live in the U.S. have limited English proficiency. Because the majority of those are Spanish speakers, many medical schools now offer medical Spanish. C.U.S.M., which was founded in 2018, has made it mandatory. Finding a common language is just one way in which medical schools, clinics, hospitals and health-care networks are working to address health disparities as part of an increasingly visible movement known as culturally sensitive or concordant care.
When patients don’t trust the providers caring for them or when they feel dismissed or misunderstood, they’re less likely to share relevant information. And when providers don’t understand a patient’s life experiences and culture or don’t speak their language, they may be less likely to ask relevant questions. Culturally sensitive care starts with the premise that people come from diverse cultural, ethnic, religious and socioeconomic backgrounds and that understanding these differences is crucial for proper health care. Hospitals and medical schools are now adding tools to help their providers improve sensitivity around language, traditions and cultural expectations. The strategy is already advancing health equity. A growing body of research shows that by addressing bias and stigma directly in a rapidly diversifying patient population, culturally concordant care results in better health outcomes across a person’s lifespan—from prenatal and maternal health to pediatrics to end-of-life decisions.
Innovations In Solutions For Health Equity
Maternal mortality rates in the U.S. are higher than in any other high-income nation in the world. In 2022 that rate was about 22 deaths per 100,000 live births, according to the Centers for Disease Control and Prevention’s National Center for Health Statistics, down from almost 33 deaths per 100,000 live births in 2021.
The death rates are the worst in Black communities. Data from the Chicago Department of Public Health revealed that in 2019, Black women in Chicago were almost six times more likely than white women to die during pregnancy or within one year of giving birth. To try to reduce this number, the University of Illinois Hospital and Health Sciences System (UI Health) introduced a new initiative in 2022: its Melanated Group Midwifery Care program.
The midwifery group was born out of Karie Stewart’s frustration with a system that was failing Black and brown families. “The Black population is experiencing the most deadly outcomes when it comes to pregnancy,” says Stewart, a certified nurse-midwife at UI Health and one of the investigators leading the Melanated Group Midwifery Care program’s research. The patients she serves are predominantly Black and live on the west and south sides of Chicago, where a number of hospitals shut down their labor and delivery units during the worst of the COVID pandemic. “There is a lack of care for those already disadvantaged,” she says. Stewart approached Kylea Laina Liese and Stacie Geller of the University of Illinois Chicago, who study risk factors associated with maternal health, and together they made a plan, secured a $7.1-million research grant and got to work.
The research project includes people at all stages of pregnancy, from the first trimester to 12 months after birth. It matches Black pregnant people with Black midwives and is expanding prenatal care in communities with limited maternal health services. The program provides group education to support people in different stages of pregnancy, offers breastfeeding resources, helps participants with family planning after their babies are born, and ultimately reframes maternal and postpartum care in a way that respects Black patients’ needs and experiences in a health-care system still recovering from historical and systemic racism.
Today Stewart and her team are four years into the five-year grant, and they can point to qualitative changes in the community they serve. (The team expects to share quantitative data after the research period ends in 2025.) “We’re seeing folks use the health-care system more. They’re not running from it,” Stewart says. “They’re empowered from their maternity experience. They’re empowered to share what’s going on.” Given that many of these patients had previously avoided the health-care system, she sees this as a big win. “We want them to be engaged in their health care not just when they’re pregnant but after having a child and to seek care for anything else they have going on.”
In medical schools across the country, clinicians, faculty, administrators and students are reviewing their curricula to identify existing biases and teach cultural sensitivity to the next generation of physicians. When schools integrated information on racial disparities into their teachings, according to a 2019 study in Academic Medicine, students were more motivated to work in diverse communities.
In 2021 Temple University’s Lewis Katz School of Medicine in Philadelphia formed a task force of students and faculty to identify potential problems in the school’s course curricula, says Abiona Berkeley, an anesthesiologist and interim associate dean of the school’s diversity, equity and inclusion office. There were 346 instances in the curriculum, she says, “where we had an opportunity for development and growth.” These included dozens of examples of racial or ethnic stereotypes, as well as symptoms that had never been studied in groups representing a range of human skin tones. Berkeley says several members of the faculty have told her, “It’s changed the way I look at some of my patients and how I engage with them.”
Hillel Maresky, a cardiothoracic radiologist, arrived at Temple University in 2019, before the cultural sensitivity task force was assembled. He soon noticed an odd phenomenon. Many of his Black female patients had chest x-rays, computed tomography scans and magnetic resonance imaging (MRI) that seemed to include shadows or squiggly lines known as artifacts. He discovered that these artifacts were being caused by the women’s hair braids, locs and twists and the hair bands that held them in place. Certain hair oils and conditioners used by Black women also presented problems: the oils occasionally contain trace amounts of metals that interfere with MRI machines’ powerful magnets. “As I was compiling these cases, I learned that there really was a hole in the medical literature on this topic,” Maresky says.
When images are unclear or contain artifacts, patients must be scanned again. And additional testing means additional radiation exposure, as well as logistical challenges such as transportation or loss of hours at work. The lack of familiarity with these hairstyles and the lack of data regarding their effect on imaging present problems not only for radiologists but for clinicians in a wide range of medical fields.
Maresky began collecting a dataset that now includes more than 100 images of such artifacts that mirrored disease, and Angela Udongwo, a fourth-year medical student in his laboratory, has now presented their findings at a couple of conferences and to other medical schools in the Philadelphia area. They have also completed a pilot study on physicians’ awareness of and familiarity with Black hairstyles. “We found the length of your career correlated with how familiar and comfortable you are with identifying these hairstyles in imaging,” Udongwo says. But these are skills that can be taught. “There is no curriculum developed around teaching this.”
Udongwo is Nigerian American and has worn braids for years. While collecting research for the project, she heard one story after another about patients who encountered radiologists with little cultural sensitivity or understanding. It just doesn’t make sense, she says, that radiologists in 2024 aren’t familiar with these hairstyles.
Medical schools are beginning to catch up. In 1991–1992, researchers surveyed all 126 medical schools in the U.S. about whether they had implemented cultural-sensitivity training or had plans to do so in the future. Their results were published in 1994 in Academic Medicine. Of the 98 schools that responded, only 13 provided a cultural-sensitivity course, and only one of those was a requirement. Today medical schools, governments and hospitals across the U.S. have guidelines for cultural-sensitivity training. They’re expanding their sensitivity around communication, too: as of 2019, almost 80 percent of the nation’s medical schools offered medical Spanish.
Not only does language concordance improve outcomes, but it can also enhance patients’ experiences. A small study by Lopez Vera assessed patient satisfaction at the Spanish-friendly Inland Empire Free Clinic and found that those treated by a doctor who spoke their language had the highest satisfaction scores. These days, between technology and artificial intelligence, some people assume they don’t need to learn a new language, Lopez Vera says. But the evidence shows that the human-to-human approach is not just more empathetic but more effective.
Many of the patients who come to Eugene Yang’s cardiology clinic trace their origins back to India, China, Korea, and multiple parts of Southeast Asia. His clinic is in Seattle, a hub for the tech industry and home to thousands of immigrant workers. Yang had seen firsthand how people from each of these groups were at risk of heart disease and how their typical lifestyles differ.
Yet despite differences in their cultures and backgrounds, these patients have been lumped together with people from other communities in a single category: Asian American, Native Hawaiian and Pacific Islander, or AANHPI. So Yang and his colleagues created a study looking at how social stress factors affect heart health in the Asian American communities he treats. The researchers analyzed stressors such as food insecurity, delays in medical care and living in a neighborhood that didn’t feel close-knit or safe. Then they correlated these issues with risk factors for heart disease among Chinese, Filipino and Asian Indian adults. Other Asian communities were grouped together into a single category.
The recently completed study showed that the same stressors manifest differently in people of different ethnicities. Across the board, those who experienced more social stress had poorer sleep, struggled to exercise and used more nicotine—all factors associated with higher rates of heart disease. But differences emerged between groups. In Chinese Americans high stress was associated with an increased risk of diabetes, whereas in Filipino adults it was linked to high blood pressure. Asian Indians were most likely to experience poor sleep and physical inactivity when bearing the brunt of social stress. “There are significant differences in how social determinants of health impact the different Asian subgroups,” Yang says. Recognizing this variation is a first step toward helping physicians tailor interventions more appropriately.
Innovations In Solutions For Health Equity
For decades such nuance had been all but invisible to scientists, clinicians and policymakers. The single AANHPI category, which was defined in the 1997 U.S. Census, is still used widely by hospitals, as well as by state and national health databases. Researchers and policymakers use these data to assess disease rates and people’s health needs and to decide how to allocate resources.
But the AANHPI category masks rich diversity. People in this group have ancestral links to more than 50 countries. They collectively speak more than 100 different languages, have widely variable ways of life that differentially affect their health risks and represent a diversity of genetic backgrounds. They’re also the fastest-growing racial and ethnic minority in the U.S. By pooling their data, researchers end up with a potpourri that obscures population-specific health needs or health risks. “When you lump everybody together, you don’t see that maybe there are important differences,” Yang says.
Now efforts led by advocates, researchers and community organizers—most of them from AANHPI communities—are paving the way to data equity and better health.
Spurred in part by the realization that aggregated data masked stark health disparities during the COVID pandemic, researchers began studying disease risk in specific AANHPI cohorts such as Pacific Islander, South Asian and Vietnamese populations. They’re finding that teasing apart data in community-specific ways lets them use race and ethnicity information without conflating it with biology. Policymakers are catching up, too, using data specific to individual communities to better understand how to allocate resources and communicate more effectively.
These efforts are improving AANHPI health outcomes, says epidemiologist Stella Yi of New York University Langone Health. In recent years disaggregating AANHPI data has helped health-care professionals improve hepatitis B vaccination rates, reduce the devastation that has been caused by COVID and wildfires among Hawaiian communities, and identify better diet strategies to help South Asian communities reduce their risk of heart disease. “It’s been really exciting to watch,” Yi says.
Tellie (Chantelle) Matagi was a 20-inch, eight-pound, six-ounce bundle of newborn joy in a Utah hospital nursery when her identity vanished into the health system. On hospital forms Matagi, who is of Samoan ancestry, had been labeled Asian, a category that blurred racial lines so completely it rendered them meaningless. Matagi, a community health leader who managed the Pacific Islander Task Force within the Hawaii State Department of Health during the early days of the COVID pandemic, says the record bothered her parents. It also troubled Asian staff at the hospital, who recognized the incongruity of so many people being lumped together. Matagi ended up quitting her job in 2022 to address her own health. She had diabetes and high blood pressure, and her doctors suggested she just lose weight. But because she was familiar with the science and knew aggregated data were masking her Samoan ancestry, she realized they couldn’t understand her true health risks. “I knew I wasn’t being seen,” she says.
Grouping too much data blurs the reality of people’s lives. For example, in the aggregate, the risk of cancer death among Asian Americans is about 40 percent lower than that for white people. But disaggregating data reveals important patterns. Within the AANHPI group, lung cancer is the leading cancer diagnosis among Vietnamese, Laotian and Chamorro (those with ancestry in the Mariana Islands) men, and colorectal cancer is highest among Laotian, Hmong and Cambodian men.
When data are pooled, these nuances vanish. “One group looks better than they really are, the other group looks worse than they really are, and you can’t rely on those estimates anymore,” says Joseph Kaholokula, a physician at the University of Hawai̒i at Mānoa. “It’s nonsense. It’s not good science, yet people have been doing this for decades.”
That’s because for decades federal and state health databases have offered researchers only a high-altitude view. Early attempts to break population data down with greater granularity failed because there simply weren’t enough people in each group. The effort sparked concerns that, although the people included in these health-related data samples should remain anonymous, there were so few they could be easily identified. And funding to look at AANHPI health has been limited—a 2019 study reported that over the previous 25 years, only 0.17 percent of all National Institutes of Health funding for clinical research supported projects focused on AANHPI communities.
This is in part the result of broader stereotyping of Asian Americans as a “model minority,” a category in which everyone is assumed to be well educated, financially secure and generally healthy. The model-minority trope illustrates how race-based assumptions can bias scientific research, says Tina Kauh, a program manager at the Robert Wood Johnson Foundation. “It’s important for people to recognize that systemic racism is really what’s driving the fact that we don’t disaggregate data.” With so little nih funding to support their work, scientists have struggled to dispel the model-minority myth. “It’s like this hamster wheel you get stuck on,” Kauh says.
Kauh first bumped into that cycle in college during an undergraduate psychology class about how culture and ethnicity shape someone’s behaviors and perceptions of social norms. Fascinated, she tried to dig deeper into the experiences of Asian Americans, yet she couldn’t find the data. Kauh persisted, revisiting the topic in graduate school but says she found it “basically impossible” to get funders interested. Since then, she says, “it’s been this mission of mine to try to push for collecting data about Asian Americans.”
Kauh’s parents were Korean immigrants who owned a convenience store in Philadelphia. Even as a teen, Kauh could tell that their grueling schedules, language issues and social isolation took a physical and mental toll. Their lives were hardly those of a model minority. “I could see the challenges they experienced on a daily basis, but no one ever really talked about that except to frame it as ‘look how hardworking they are,’” she says.
The social stressors Kauh’s parents experienced were financial and cultural, both of which can affect a person’s health. Language barriers, racism, changes in diet with the move to a new country and the circumstances of that move—whether someone migrates to pursue a graduate degree or to flee from conflict—can add up. None of these factors are related to the biological basis of disease, but they determine what resources a person or community might need to achieve good health.
Source Zhu, A. L. et al. J. Am. Heart Assoc. 13, e032509 (2024). Graphic by Jen Christiansen
When researchers understand the links between social factors and people’s health, they can begin to design tailored solutions. Food is one clear example. In the U.S., South Asian communities have disproportionately high rates of heart disease—an observation often explained by diet, says Alka Kanaya, a clinician who studies diabetes at the University of California, San Francisco. Researchers typically gather details about food habits using a list of standard questions based on Western diets that don’t represent global cuisines. Advice about what constitutes a “healthy” food is also based on studies conducted with Western diets. “You have to be specific to what people may be eating and how they may be cooking it. Having nonaccurate ways of measurement just gives you useless data,” Kanaya says.
For the past decade Kanaya and other researchers have run a study of heart health among South Asians living in the U.S. called Mediators of Atherosclerosis in South Asians Living in America (MASALA). It includes a food-frequency questionnaire that lists many South Asian foods, such as dhokla (a savory cake), sambar (lentil stew), steamed fish, lamb curry and popular snacks. Last year the researchers analyzed the diets of nearly 900 people from the study and identified foods correlated with a “South Asian Mediterranean-style diet”—one rich in fresh vegetables, fruit, fish, beans and legumes. They found that people who ate more of these foods had a lower risk of heart disease and diabetes than other people in the cohort.
Data such as these can help clinicians advise patients more effectively by offering dietary solutions that may be easier for them to follow rather than forcing a more Western lifestyle on them, Kanaya explains.
Getting granular with community data proved to be a lifesaving strategy in Hawaii during the worst of the COVID pandemic. The state health department’s infectious disease team was heavily focused on controlling the spread of the virus at the start in 2020. But the scientists were “thinking of it in terms of a purely biological system versus understanding what puts people at risk,” says Joshua Quint, an epidemiologist at the Hawaii State Department of Health. “Accurate measurement of social factors is so important.”
To gather those data, Quint teamed up with Matagi and Kaholokula, the University of Hawai̒i physician, to form a COVID investigation team. The group quickly discovered there was no way to figure out which of the Native Hawaiian and 20 or more Pacific Islander communities needed resources or what those resources were. The data at hand were simply too sparse to base any estimates on. So the team began recording COVID deaths with more specific demographic details. When counts were low enough that they risked making individuals identifiable, the team noted these details in a separate section of the database to ensure that information from smaller communities was not lost in an aggregate, Matagi says.
The team members didn’t just gather information—they shared it with the communities through hours of virtual visits and phone calls. As they talked, the carefully gathered and stored details helped communities see their own losses amid the sea of numbers. No one could deny the devastation they’d experienced, nor could their experiences be minimized by a database that didn’t represent them and their needs. The strategy was especially effective among the Samoan, Marshallese and Chuuk (people originally from part of Micronesia), Matagi says, because they were the three Pacific Islander communities most affected by the disease.
The researchers worked with each community to identify specific requirements. Some needed a safe place to keep healthy family members distanced from those with COVID, others wanted more resources allocated to food or medical care, and still others sought a way to maintain social connections or attend religious gatherings virtually while observing COVID precautions.
The same approach helped the team customize care after the Maui wildfires by recognizing specific needs such as food, shelter and medicine. Its methods have since been highlighted by the World Health Organization as an effective way to reduce health disparities.
Identifying a community’s needs and meeting them appropriately can make a range of infectious diseases more manageable. In New York City in the early 2000s, routine hepatitis B vaccination was available only to children. Among adults the virus was typically seen as a sexually transmitted infection (STI), and testing and treatment were offered primarily at HIV clinics.
But the infection was common among Asian American immigrants because of high endemic rates in their countries of origin. In families the virus passed between married partners, from person to person through household contact such as the sharing of utensils, and from mother to child during childbirth. These adults were unlikely to seek care at an STI clinic. At the time, researchers reported rates of hepatitis B among Asian Americans that were about 50 times higher than those among non-Hispanic white people, as well as rates of liver cancer, a common consequence of infection, that were several times higher. In 2003 researchers at New York University teamed up with community organizers, politicians and clinicians in the city to help address the disparity.
The coalition’s work helped to establish that the problem would not be stemmed by STI clinic screenings, because that “was not somewhere that we knew Asian American immigrant adults would feel comfortable going,” says epidemiologist Simona Kwon of N.Y.U. Langone Health, who joined the effort a few years after it began. “The communities are very different,” Kwon says, “and the health priorities are different.” Western social norms and biased perceptions had been unintentionally driving health outcomes for hepatitis B.
The N.Y.U. team helped city officials implement community-based programs and offer adult vaccinations at primary care clinics and through community-based organizations. Recognizing that not just viral infection rates but social conventions guide people’s choices about care was the key to driving down hepatitis B transmission.
Quint warns that in efforts to apply race and ethnicity data, researchers and policymakers should be careful not to conflate a person’s health with these factors alone. Aggregated or not, race and ethnicity are always simple representations of broader social and cultural factors that affect health. But disaggregation, he says, can “help us get beyond race and talk about ethnicity in ways that are more meaningful and helpful.”
Efforts to create community-specific solutions are what “actually move the disparities dial,” Matagi says. Now, after the success of state- and community-level studies, policymakers are launching larger studies and investing more money in the hopes of better understanding the health of different groups under the AANHPI umbrella.
Last year the White House announced a national effort to prioritize equity for AANHPI communities, and earlier this year the National Heart, Lung, and Blood Institute launched a large epidemiological study to understand health trends in these populations. This seven-year project, named the Multi-ethnic Observational Study in American Asian and Pacific Islander Communities (MOSAAIC), aims to track the health of 10,000 people who identify with various AANHPI subgroups. One challenge, Kanaya says, will be to find out how granular they can get—keeping the data anonymized but with sufficient detail to identify meaningful trends, yet without adding so many checkboxes that a long list leaves participants exhausted.
Establishing new categories of race and ethnicity may seem to contradict efforts to make medicine and health care equitable and free of racial bias. But done right, these endeavors can be complementary. “There’s a push to avoid talking about race, and I think there are big risks associated with that if it’s coming from a place of wanting to ignore problems,” Quint says. “We need statistics that cut across all ranges of demographic factors so we can find out if we’re building a more just and fair society.”
The abandoned buildings behind the New Somerset hospital in Cape Town, South Africa, are prime real estate along the waterfront, so guards patrol the area day and night to protect against squatters. But squatters aren’t the only visitors. Tucked in among the empty facades is the Ivan Toms Center for Health, one of the first clinics in South Africa for men who have sex with men. It was launched in 2009 to provide comprehensive, free and sensitive health care. These days a new concern is on the minds of its visitors: mpox.
The first human case of mpox, formerly known as monkeypox, was described in the 1970s. The disease is thought to be caused by a virus that jumped from animals to humans and causes symptoms similar to smallpox. This past August the World Health Organization designated mpox a public health emergency of international concern for the second time in two years. Although the risk of mpox is not limited to men who have sex with men, the transmission dynamics of the 2022 outbreak led researchers and public health officials to identify them as a high-risk group. During 2022 more than 90 percent of known cases were among gay, bisexual, and other men who have sex with men. As the outbreak builds, Ivan Toms and similar clinics have seen an increase in patients wanting information.
Epidemics begin and end in communities. Today people around the world understand and respond to outbreaks differently than they did before the COVID pandemic. They appreciate concepts of transmission, protection and vaccine availability at a deeply personal level and are hungry for information. They want to know if a case has appeared locally and, if so, how to protect themselves. And the community most affected by mpox is one that has suffered multiple other outbreaks—most notably, the HIV/AIDS crisis. Critically, that means it’s a community that clinicians and public health researchers know, understand and collaborate with.
Innovations In Solutions For Health Equity
Dimie Ogoina, a Nigerian infectious disease physician-scientist, and his team were the first to describe sexual transmission of mpox in Nigeria in 2017. He believes that what makes the disease so challenging is the comorbidities that exist in Africa, especially co-infection with HIV. His team noticed that those with the most severe cases of mpox also had HIV infections. “Most of them had advanced HIV … and [were] not on treatment,” Ogoina says.
People with HIV accounted for around 40 percent of those diagnosed with mpox in the 2022 outbreak, and recent studies suggest that people who have more advanced HIV have worse clinical outcomes and higher mortality from mpox. How the two diseases interact is still a mystery, however. Researchers have yet to tease apart whether HIV infection raises the risk of acquiring mpox or increases its severity or whether people living with HIV simply might be more likely to be diagnosed because they’re already receiving better care. Better understanding this connection could be critically important. As the outbreak spreads to more nonendemic countries, effective treatment of HIV could hold one key to bringing the outbreak to an end.
Mpox’s present echoes HIV’s past—it’s a disease that has the potential to affect everyone and is more dangerous within a specific community. The comparison is etched in the brick and mortar of the clinic on the waterfront: Ivan Toms, the man, was both an anti-Apartheid and a gay rights activist.
The challenge with both diseases is how to get information to an already stigmatized group of people in a timely enough manner to halt the ongoing outbreak without making that stigma even worse. The 2022 outbreak showed that our first attempts failed: an article in PLOS Global Health was simply entitled “Monkeypox Is Not a Gay Disease,” recognizing that stigma had quickly emerged around the virus, echoing the early days of the HIV pandemic.
The advantage today is that those dealing with mpox have lessons from HIV/AIDS to follow. One small but meaningful way this has already been addressed is its name: monkeypox was renamed in 2022 to mitigate against racist and stigmatizing language. And as a result of the 2022 global emergency and lessons learned from the HIV/AIDS pandemic, public health officials are better equipped to build coordinated messaging and meet patients where they are.
“[Our] clients overall are now familiar with mpox, as we had the 2022 outbreak and did extensive education,” says Johan Hugo, an HIV clinician at the Ivan Toms Center. The center has integrated mpox services into its HIV care as recommended by the WHO and is part of a network of clinics and government agencies, including the South African Department of Health, that are using common messaging and strategies for mpox. “We work closely with organizations that support key populations to ensure we remain in line with one another,” he says. Such coordination in messaging helps to combat stigma around a disease that is not yet fully understood.
Despite significant improvements in access to HIV/AIDS treatment, gaps persist because patients are worried about their diagnosis creating stigma related to sexual and reproductive health. It is no different with mpox. The stigma associated with mpox can adversely affect prevention and treatment, with people less likely to disclose symptoms or seek care—they may even hide their condition for fear of being diagnosed. There is no specific treatment for mpox, and its symptoms are similar to those of other viruses such as chicken pox. But rapid, accurate diagnosis is the only way to prevent transmission and end outbreaks.
To achieve this, public health officials are taking everything they’ve learned from HIV and using it to attack mpox outbreaks. For instance, Ivan Toms and other clinics have developed approaches for delivering health services that allow for discretion and privacy. In addition to onsite testing and health checks, the center also packages and dispenses medications for its clients, eliminating the need to visit a general pharmacy. The approach has been so successful that after becoming the first clinic to run demonstration projects for HIV Pre-Exposure Prophylaxis (PrEP) in Africa in 2015, Ivan Toms is now one of the largest providers of PrEP in South Africa and a key training institution for service providers across 11 African countries.
PrEP reduces HIV risk by preventing HIV from entering the body and replicating. But protection requires that users maintain high levels of the medication in their bodies. Because adherence is crucial, practitioners aim for frictionless care that removes any social barriers. To that end, the clinic runs a WhatsApp service, smart lockers that safely store patients’ medicines, and mobile units that go directly into communities. Across the entire Cape Metro area, mobile units provide comprehensive HIV testing, treatment and prevention services, including self-screening, PrEP, antiretroviral drug initiation and follow-up, viral load testing, and screening for sexually transmitted infections. “Our mobile units are an extension of our facility and seek to provide the same level of care,” Hugo says. “Each of our teams provides comprehensive HIV testing, treatment and prevention.”
Because so many men who have acquired mpox are using PrEP, researchers think HIV may simply be another marker of higher-risk behaviors facilitating infection. The goal will be for mpox services to follow the same community outreach. “Our strategy for mpox currently is to provide broader information online and then to ensure that every client who comes through our services is provided direct information about the current situation,” Hugo says. Most days, that’s as many as 120 to 150 people.
There are two variants of mpox virus: clade I is endemic to central Africa and has killed up to 10 percent of the people it has infected during previous outbreaks, making it far deadlier than clade II, the type responsible for the 2022 outbreak. Both are circulating today in different countries in Africa. And unlike the 2022 outbreak, this one—which is tearing through the Democratic Republic of Congo (DRC)—has largely spread through men seeing women who are sex workers. “We are not dealing with one outbreak of one clade—we are dealing with several outbreaks of different clades in different countries with different modes of transmission and different levels of risk,” said Tedros Adhanom Ghebreyesus, WHO’s director general, during his opening remarks at the emergency committee meeting where the global health emergency was declared. “Stopping these outbreaks will require a tailored and comprehensive response, with communities at the center.”
In July 2024 South Africa notified the WHO of 20 confirmed mpox cases between May 8 and July 2, including three deaths—the first reported in the country since 2022. Cases occurred in three of South Africa’s nine provinces, including the Western Cape, where the Ivan Toms Center for Health resides. How the outbreak evolves from here will depend heavily on case identification and treatment management.
There is one internationally approved vaccine for mpox (another is approved in Japan with emergency approval in the DRC), which can act as both preexposure and postexposure prophylaxis for people at high risk. But although the vaccine is available in numerous high-income nations, current access in South Africa is limited to nonexistent. “The vaccine was originally made for smallpox, with U.S. funding,” says Mohga Kamal-Yanni, a senior policy adviser to the People’s Medicines Alliance, a global coalition with the goal of creating equitable access to vaccines and other medical technology. The companies that make these vaccines hold their patents, she says, “and when the mpox outbreak started, there was no discussion on technology transfer to another potential manufacturer.”
During the COVID pandemic, African countries surpassed all expectations despite challenges in vaccine access. Tanzania emerged as one of the best-performing African countries for COVID vaccination rates: Between January 2022 and April 2023 the country managed to bump its total population vaccination rate from 2.8 to 51 percent. This happened in part because COVID-specific vaccinations were integrated with other routine health services, allowing for effective delivery.
The COVID pandemic forever changed Africa’s policy, regulatory and vaccine landscapes. Low-income countries have learned to push through regulatory red tape, advocate for their people and work with high-income nations to get vaccines distributed more equitably. After putting a vaccination plan in place, Nigeria received the first donation of 10,000 vaccines from the U.S. just a few days after the global mpox emergency was declared. Other donations are aimed at countries across the African continent: Spain promised 500,000 doses from its stockpile, the U.S. committed to sending another 50,000 doses to the DRC, and Japan pledged millions of doses. Some of those vaccines have already arrived in Africa.
Citing lessons learned from COVID, global health institutions are also mobilizing resources. Gavi, the Vaccine Alliance, has mobilized resources for mpox, the rollout of which will be an early test of Gavi’s First Response Fund. The fund aims to make resources immediately available for a vaccine response to a public health emergency and includes a $500-million fund aimed at ensuring early access to vaccines within days of an emergency declaration. This, according to Gavi director of development finance David Kinder, was one of the big lessons learned from COVID.
The 2022 mpox outbreak was deemed to be over about nine months after the WHO declared an emergency. The 2024 outbreak could be larger and longer. If it is going to be extinguished as quickly, lessons learned from previous pandemics hold the key.
The country someone is born into has a lifelong effect on their health. So does the neighborhood they live in, the color of their skin, their income and their level of social support. It’s unjust. After centuries of persistent health disparities, researchers, advocates, clinicians and public health experts are finding ways to improve health for everyone.
Innovations In Solutions For Health Equity
New advances sometimes exaggerate inequities before helping reduce them. But there are reasons for optimism, which journalist Anil Oza shares in a feature. More than almost any other development, vaccines have advanced health equity around the world. They have averted 154 million deaths over the past 50 years, a life saved every 10 seconds, as health writer Tara Haelle explains. Collaborative campaigns have brought this powerful preventive health care to children in even the most impoverished regions. Writer Carrie Arnold shows how rural areas around the world are benefiting from other inventive and resourceful ways to deliver needed care—from telemedicine to micro clinics to a traveling dialysis bus.
Researchers are working to remove racial bias that has been built into diagnostics, and by doing so they’re changing not just tools and algorithms but lives. As journalist Cassandra Willyard writes, some Black patients once deemed ineligible for new kidneys, despite having the same laboratory results as white patients, are now moving up the wait list for transplant; others with respiratory issues might be able to file for disability after previously being judged unqualified. Epidemiologists and other public health scientists are discovering that prior assumptions about race have lumped together disparate groups with different needs and health risks, particularly within Asian American communities. Now, by teasing apart the data, they are able to better diagnose, treat and even prevent disease. Health writer Jyoti Madhusoodanan reveals how this data-driven approach is already saving lives.
Certain diseases and conditions have been used to justify discrimination, especially when the disease is more prevalent in a group that’s already marginalized. The people most at risk for mpox, for instance, are men who have sex with men—a community already hit hard by HIV/AIDS. But as global health expert Charles Ebikeme writes, researchers, clinicians and community members have learned from past experiences and are building up existing networks and clinics that cater specifically to this stigmatized population. Even health-care communication is improving, writer Rod McCullom shares in a feature, as the movement toward culturally sensitive care helps clinicians better understand and empathize with their patients.
Improving health equity requires rethinking our global health infrastructure, and we are still at the beginning. But each solution adds support and begins to build a path toward justice.
Melanie Hoenig was teaching first-year medical students how to estimate kidney function when one of them, Cameron Nutt, raised his hand. Why, he asked, did the diagnostic algorithm include an adjustment for Black patients? In the U.S., Black people have higher rates of kidney disease and kidney failure and are less likely to get a kidney transplant than white people, but the adjustment makes it seem as though Black people have better kidney function than people of other races who have the same test results.
Good question, thought Hoenig, a kidney specialist at Beth Israel Deaconess Medical Center in Boston. She had never wondered why this might be. “I said, ‘You’re right. That doesn’t make any sense,’” Hoenig recalls of the 2016 classroom conversation.
This value for kidney function, called the estimated glomerular filtration rate (eGFR), helps doctors figure out when to send patients to a specialist, when to start dialysis, when they are eligible to join the wait list for a kidney transplant, and where their name lands on that list. Adjusting the algorithm for Black patients decreased their chances for treatment and transplant.
Innovations In Solutions For Health Equity
The equations and instruments doctors rely on are infused with historical bias. Medicine has long treated race as though it provides important information about the underlying biology and genetics of disease, a strategy that has had an enormous impact on diagnosis and treatments. People have been passed over for kidney transplants, denied therapies and diagnosed with diseases later than necessary simply because of the color of their skin.
Race is a social construct that reveals little about ancestry. There is more genetic variation within racial groups than between them. “The racial differences found in large datasets most likely often reflect effects of racism—that is, the experience of being Black in America rather than being Black itself,” researchers wrote in a 2020 New England Journal of Medicine article outlining the dangers of race-adjusted algorithms.
To undo this bias, researchers are changing the algorithms and instruments and finding new models to reduce disparities.
Kidneys filter waste and excess water from the blood through tiny structures called glomeruli. Directly measuring how well these glomeruli are functioning is possible but cumbersome, so instead doctors rely on blood levels of a protein called creatinine, a waste product produced by muscles and a by-product of protein metabolism, to estimate the glomerular filtration rate (GFR). When kidneys are working well, they filter out creatinine; if the kidneys start to fail, creatinine levels rise. The protein is easy and inexpensive for laboratories to measure.
The first equation to assess kidney function, developed in the 1970s, relied on age, sex, weight and creatinine levels in the blood. But the formula wasn’t precise. So, in the late 1990s, a team of researchers set out to develop a more accurate one. They used existing data from a study of creatinine and GFR in more than 1,600 people, then correlated the two measurements. The team looked at 16 different factors that might influence the relationship. (We tend to lose muscle mass as we age, for example, so older people have lower creatinine levels than younger people.) The authors noted that for any given GFR, creatinine was higher in Black people than in white people. Why that might be wasn’t clear. Maybe it was because Black people had higher muscle mass, they speculated. The study population was only 12 percent Black, yet the difference felt too substantial to ignore.
To account for this difference, the researchers added an adjustment for Black patients: a multiplication factor of up to 1.21, which essentially inflated their estimated kidney function by as much as 21 percent. In 2009 the researchers published an updated equation, but the Black correction factor remained, albeit lower, up to 1.16. “We always recognized that race was not the biological process by which African Americans differed from non–African Americans in the relationship between GFR and creatinine,” Andrew Levey, who worked to develop both equations, later explained. But “it stood in for something that was important.”
“The way the lab report was written was, if your creatinine is a 4.0, your kidney function is 19 percent. Oh, unless you’re African American; then it’s 22 percent,” says Martha Pavlakis, a nephrologist at Beth Israel Deaconess. “It makes no sense.” In people with healthy kidneys, small differences don’t matter. But when kidney function declines, eGFR, which decreases as blood creatinine levels rise, becomes crucial. That number helps to determine whether a patient is referred to a nephrologist, diagnosed with kidney disease or deemed eligible to join the wait list for a kidney transplant.
Hoenig began working with a small group of students from Harvard Medical School’s Racial Justice Coalition to lobby to eliminate the correction factor, and in 2017 Beth Israel Deaconess became the first medical center to do so. Efforts elsewhere largely stalled until the deaths of George Floyd, Ahmaud Arbery and Breonna Taylor, three Black Americans whose deaths made national news. In the wake of their killings, conversations about race rippled throughout the medical community, Pavlakis says.
As protests erupted across the country, medical students and faculty at many major universities began to circulate petitions calling for an end to the use of the racial correction in eGFR. Some major academic health systems began removing race from the equation, but their approaches were inconsistent. Neil Powe, chief of medicine at Zuckerberg San Francisco General Hospital and Trauma Center, and other experts watched the changes unfold with concern. There was no unified way of diagnosing kidney disease. “You could be at one hospital and have a diagnosis of kidney disease. You go down the street [to another hospital], and you wouldn’t have kidney disease,” Powe says. “That was just chaos.”
In the summer of 2020 the National Kidney Foundation and the American Society of Nephrology formed a task force to assess how best to move forward. “They thought we’d solve it overnight, but it took us about 10 to 11 months to churn through this,” says Powe, who co-led the task force. Ultimately they chose an equation that used the same 2009 data but eliminated race as a variable, then refit the curve to the whole dataset.
A conversation about race was also happening at the Organ Procurement and Transplantation Network (OPTN), which manages transplants from deceased donors. The wait list for a kidney is long. Patients aren’t eligible to join until they meet certain criteria; these can vary at different transplant centers, but all candidates must have an eGFR of 20 percent or less. And because of the eGFR correction factor, Black patients needed higher creatinine levels than people of other races to pass that threshold. “Nobody who came up with the formula was like, let’s keep Black people off the list. But that, in fact, was the result,” Pavlakis says.
In July 2022 the race variable was explicitly forbidden in organ allocation. Pavlakis saw that as just the first step. She wanted to help Black patients already on the list and those who had previously been denied entry because of their kidney function numbers.
In January 2023 the OPTN decided that transplant centers should look back at the lab reports of Black patients on the list and recalculate their eGFR using the race-neutral equation to see whether they should have been referred for transplant. “Basically, half the Black patients on the transplant list got extra priority added to their standing because of this project,” Pavlakis says.
Pavlakis acknowledges that this change doesn’t fix every disparity in kidney allocation. But she also sees it as restorative justice. “It’s not perfect,” she says, but “I think it’s probably the largest example of fixing a race disparity that is out there.”
Pulmonologists have been grappling with a similar problem. To assess lung function, doctors ask patients to blow into a device called a spirometer, which measures the maximum amount of air a person can exhale and how much they can force out of their lungs in a single second. The spirometer compares those numbers with reference values for “normal” lung function. The results help doctors diagnose diseases such as emphysema and chronic obstructive pulmonary disease, assess severity of those conditions and monitor declines in lung function.
What constitutes “normal” varies by age, sex, height and, until recently, race. Why race? Data collected in the late 1800s and early 1900s suggested different races have different lung capacities, a phenomenon researchers ascribed to innate biology rather than social, economic or environmental factors. By the early 20th century the idea that lung capacity varied among racial groups was “an ostensible fact,” wrote Brown University researcher Lundy Braun in a 2015 article on the historical use of race in spirometry. What experts missed was that race was probably a proxy for other factors, such as air quality, nutrition, and other exposures, that affect lung health and development.
When the European Respiratory Society’s Global Lung Function Initiative developed reference values for spirometry in 2012, it used more than 160,000 spirometry results from 33 countries. Researchers observed “proportional differences in pulmonary function between ethnic groups” and decided to develop separate values for four groups: Caucasian, African American, North Asian and Southeast Asian. They also used an “other” category for people who didn’t fit elsewhere. The model assumes that, compared with white adults, Black adults have about 10 to 15 percent smaller lung capacity and that adults of Asian ancestry have 4 to 6 percent smaller lung capacity. So the same spirometry results in Black, Asian and white people led to different interpretations of health. As a result, lung diseases in certain populations have gone undiagnosed and untreated.
The division of reference values by race is problematic for many reasons. “We’re a big melting pot,” says Alexander Niven, a pulmonologist at the Mayo Clinic in Minnesota. So even if there were “a specific cluster of genes that predispose people to greater or less lung function, that’s highly unlikely to remain a pure cluster in this global world.”
What’s more, lungs are in constant contact with the outside world and continue developing throughout childhood and into early adulthood, Niven says. “It’s impossible to separate race from all of these other factors that unfortunately are inexplicably linked to different populations within our society, many of which are likely coloring the changes in lung function that we see in different social groups.”
In practice, the race-based model doesn’t seem to improve predictions when it comes to outcomes that matter. “You can’t tell any better who’s going to go to the hospital. You can’t tell any better who’s going to die. You can’t tell any better who has severe symptoms and who doesn’t. And in some of those cases, you actually worsen your ability to predict by adding race,” says Aaron Baugh, a pulmonary and critical care physician at the University of California, San Francisco.
In 2023 the Global Lung Function Initiative replaced race-based equations with a race-neutral equation. That same year the American Thoracic Society and the European Respiratory Society recommended all health-care providers switch to the new formula.
That shift is happening now, and researchers are just beginning to uncover the broad impact of this change. “Long story short, it’s profound,” says Arjun Manrai, a bioinformatics researcher at Harvard Medical School. Lung function helps to determine disability payments, candidacy for some professions, priority for lung transplants, and more. Manrai and his colleagues found that some 10 million people in the U.S. would have their diagnosis or the severity of their disease reclassified. Disability payments could increase by more than $1 billion. Such changes are not always beneficial. A new diagnosis can make someone ineligible for certain jobs, such as firefighting. And a Black person with lung cancer might not be identified as a good candidate for surgery because their lung function may be too poor to allow for removal of part of their lung. “There are trade-offs essentially attached to these reclassifications,” Manrai says.
The new equation comes from the same 2012 data as the original formula, and it isn’t perfect. “We kind of settled on the race-neutral equations we have now as the best current option, knowing that in the future, something better might arise,” Baugh says.
Manrai thinks a lot about how traditional algorithms operationalize race, adjusting what constitutes “normal” for any particular patient, and how lessons from those algorithms can be incorporated into producing more sophisticated machine-learning algorithms. “They can be biased, and they can propagate the very same sort of race-based medicine,” he says. “But they’re a tool, and the tool can also be used in the reverse direction: to mitigate existing disparities and to potentially reduce existing biases in the health-care system.”
One example of how AI might help improve health equity is evident in research on disparities in knee pain. Previous studies have shown that Black people routinely report more intense knee pain from arthritis than people of other races. But often that pain can’t be explained by the structural damage visible in x-rays. As a result, it is often dismissed or attributed to external factors such as psychological stress.
Emma Pierson, who studies machine learning and health-care inequities at Cornell University, and her colleagues wanted to understand whether there might be physical signs in the knee itself that could explain this pain disparity. They used knee radiographs and patient pain scores from more than 4,000 people who had osteoarthritis or were at risk of developing it to train a machine-learning model.
Surprisingly, the model predicted pain better than the traditional arthritis scoring system. Specifically, Pierson says, “it seems to be picking up on factors that disproportionately affect underserved patients.” What those factors might be isn’t clear, and Pierson emphasizes a need for caution. “In general, the capabilities of these models tend to outstrip our ability to understand how they’re achieving those capabilities,” she says.
Sometimes diagnostic instruments introduce bias. The fingertip clamps doctors use to measure oxygen levels in the blood, for example, work by measuring the absorption of different wavelengths of light to estimate the blood oxygen level. But the device, called a pulse oximeter, tends to overestimate oxygen saturation in people with darker skin tones.
Researchers have known about this problem for decades, but manufacturers didn’t feel much pressure to fix the problem. The effect was relatively minor, and it was most prominent at low oxygen saturations. “That difference was probably correctly assumed to not be physiologically relevant,” says Michael Lipnick, an anesthesiologist at the University of California, San Francisco, who leads a research project to assess pulse oximeter performance. “If somebody’s oxygen saturation is really 1 percent or even 2 percent higher or lower than the real value, there’s no harm.”
When the COVID pandemic sickened millions of people, however, small biases had an outsize effect. “Clinical decisions were being made based on that number,” Lipnick says. In 2023 a team of researchers looked at health records from more than 24,000 people hospitalized with COVID during the first 19 months of the pandemic. They zeroed in on those who had both a pulse oximeter reading and an arterial blood gas test, the gold standard for measuring oxygen saturation in the blood. Pulse oximeter readings consistently overestimated oxygen levels in Black and Hispanic patients. Black patients were also more likely than white patients to have their need for COVID therapy underestimated because of inaccurate pulse oximeter readings. Such oversight has clinical consequences: being passed over for COVID treatment resulted in an hour’s delay in care on average and a higher risk of readmission.
Lipnick is part of the Open Oximetry Project, which has been testing different pulse oximeters in diverse groups to get a sense of their real-world performance. He and his colleagues have seen a range of variability. Most devices tended to perform worse when used on people with darker skin pigment, but some performed better.
Researchers are working to develop more accurate tools, and regulators are considering larger test populations with a variety of skin tones. Lipnick wants better pulse oximeters but worries that some of the fixes may increase costs. “It’s a big concern, especially in low- and middle-income countries, where the majority of the world’s people with darker skin pigment live,” he says.
In the short term, Lipnick says, clinicians should rethink how they use data from pulse oximeters. “It gives a number, and we assume that that number is truth.” In reality, the number might be off by as much as 5 percent. If doctors recognize the error rate, they can make decisions that aim to minimize health-care disparities. “I think a lot of the solution will lie in how we use the technology,” he says.
Pavlakis also sees a need for more critical thinking on the part of clinicians. She is dismayed at the number of years that she relied on the eGFR equation without stopping to carefully consider the rationale for its race correction. “When we were taught this formula, we were like, ‘This is data-driven. This is from a research study. This must be accurate,’” she says. Evidence-based, however, doesn’t always mean equitable, and that’s the real goal. Hoenig’s students and other people who recognized bias are making health care better for all.
Once a week, early in the morning, community health worker Kiden Josephine Francis Laja mounts her bicycle and pedals as far as 10 miles away from her small village in South Sudan. Some weeks Laja is doing outreach, spending her day educating a community about which vaccines she can provide and what diseases they prevent. “It’s my responsibility to tell the mothers to bring the children for vaccination,” she says. She answers their questions and lets them know she’ll be back, usually the following week, to vaccinate their children. Late in the evening she mounts her bike and heads home.
When Laja returns with the vaccines, kept in a cooler with ice packs, she will spend the day immunizing anywhere from a few to 200 children against a range of diseases: polio, tetanus, diphtheria, pertussis, hepatitis B, influenza, bacterial meningitis, tuberculosis and, more recently, COVID. Most people in high-income countries haven’t seen these diseases in decades, but the people of South Sudan know them well. Many have seen family and friends die from them.
During the rest of the week Laja works at the community health center in her village of Pure, monitoring the solar-powered refrigerator and the vials inside. She vaccinates anyone who comes to the facility and metes out drugs for a few maladies such as ulcers, malaria and typhoid. But the village doesn’t have antibiotics—or electricity. Villagers grow their own food, raise goats and chickens, and get their water from wells in the ground.
Innovations In Solutions For Health Equity
It’s not easy work for just $102 a month, especially when it sometimes takes three months for the 25-year-old mother of two to get her pay. When it rains on travel days, she and her outreach pamphlets get soaked. She must regularly check the temperature of the vials in the cooler and replace the ice packs at just the right time to ensure the vaccines don’t go bad.
People in South Sudan don’t have much, but they have this program. “Vaccines are very important to me and my community and even to my country,” Laja says. During a large outbreak of measles that began in 2022 in the country, thousands of children suffered from the disease, and many died, leading to a nationwide vaccination campaign in 2023. “Now in our community you cannot find cases of measles,” she says.
Around the globe the measles vaccine has saved nearly 94 million lives over the past 50 years. This and other vaccinations have revolutionized global health. “Immunization is the most universal innovation that we have across humankind,” says Orin Levine, a fellow at the Center for Global Development in Washington, D.C. He notes that there are people around the world without access to telephones or even toilets, but they find ways to get their children immunized. “It’s the innovation that demonstrates what is possible in terms of delivery of service to everyone everywhere.”
A May study in the Lancet estimated that vaccines against 14 common pathogens have saved 154 million lives over the past five decades—at a rate of six lives every minute. They have cut infant mortality by 40 percent globally and by more than 50 percent in Africa. Throughout history vaccines have saved more lives than almost any other intervention. And vaccines’ promotion of health equity goes far beyond preventing death. The Lancet study found that each life saved through immunization resulted in an average 66 years of full health, without the long-term problems that many diseases cause. Vaccines play a role in nearly every measurement of health equity, from improving access to care, to reducing disability and long-term morbidity, to preventing loss of labor and the death of caretakers.
“We say vaccines are one of humanity’s great achievements in terms of having furthered the lifespan and life quality for humanity in the past 50 years,” says Aurélia Nguyen, chief program officer at Gavi, the Vaccine Alliance, a public-private partnership that works to ensure low- and middle-income countries have access to vaccines against more than 20 infectious diseases. Of all the different health interventions that exist, she says, “vaccines have the widest reach across the world.” The clearest evidence of vaccines’ impact on equity is that they are often the first intervention introduced into a community with no other health-care resources.
“When you don’t have a health worker or health system, there’s nothing. If you have no money, then you want the best bang for the buck, and it’s going to be immunization,” says Seth Berkley, former CEO of Gavi. “For every dollar you invest in immunization, you get $54 of benefit. From a cost-effectiveness point of view, it’s the best investment, so it tends to be the intervention that gets out to those communities first. And once you do that, you have a health worker who’s visiting those communities on a regular basis, and then that begins to start the conversation toward more primary health care, and that leads to getting a basic clinic set up. Immunization is the vanguard of the health system.”
Every country in the world has an immunization program thanks to the World Health Organization’s Expanded Program on Immunization, which was established in 1974. “Every single country and territory” has access to at least some vaccines, says Kate O’Brien, director of the WHO’s immunization, vaccines and biologicals department. Poverty, malnutrition, underlying health conditions, overcrowding, human conflict, displacement, and lack of access to medical care, hygiene or sanitation—all of these are risk factors for infectious disease, O’Brien says. Vaccines’ ability to reduce disease in the settings most plagued by these problems gives them disproportionate power to improve equity.
There may be no greater demonstration of vaccines’ power to deliver health equity than their success with smallpox. “The magnitude of the accomplishment of having eradicated smallpox, where absolutely nobody on this earth gets the disease,” O’Brien says, “that’s the ultimate in the issue of equity.”
A version of a smallpox vaccine was developed in 1796, and in 1959 global health experts decided to pursue full eradication. In the decade that followed, it became clear that such an ambitious goal would require more than political will. Although smallpox had been eliminated from North America and Europe, frequent outbreaks continued in South America, Africa and Asia.
In 1967 the WHO started its Intensified Eradication Program, which prompted a series of innovations. The bifurcated needle, which was developed around that time, allowed for smaller doses and required less user expertise for vaccine delivery than the previously favored jet injector. Researchers created a surveillance system to better track disease and vaccinate close contacts of infected people, making mass vaccination campaigns more effective. The last documented case of smallpox occurred in Somalia in 1977, and the WHO declared smallpox officially eradicated three years later.
That success inspired a similarly lofty goal in 1988 that has proved far more challenging: eradicating polio. Since the establishment of the Global Polio Eradication Initiative, cases have fallen 99 percent worldwide, but that last 1 percent is taking decades longer than planned. Public health experts now recognize that very few diseases can be completely eradicated through immunizations. Even so, they aim to decrease vaccine-preventable diseases to such low levels that severe morbidity and mortality are negligible. The WHO’s renamed Essential Program on Immunization initially focused on six childhood diseases: polio; measles; disseminated tuberculosis, the form of the disease most common in children; and diphtheria, tetanus and pertussis, for which children receive the combined DTP vaccine. It has now expanded to include vaccines against 13 diseases.
Source: Shattock, A. J. et al. Lancet403, 2307–2316 (2024). Graphics styled by Jen Christiansen
Source: Shattock, A. J. et al. Lancet403, 2307–2316 (2024). Graphics styled by Jen Christiansen
“We have to look backward, in some ways, to realize how far we’ve really gone,” says Lois Privor-Dumm of Johns Hopkins University, who recently retired from her role as a senior research associate. “There has been tremendous progress over the past 50 years, and what is really left is making sure the equity agenda is really a focus.”
Now the question is how best to do it. A raft of technological and policy innovations aim to help. Before the WHO’s current vaccination program began, fewer than 5 percent of the world’s babies had access to routine immunizations. Today 84 percent of infants have received three doses of the DTP vaccine, the metric used to assess global immunization coverage.
“[Vaccines] level the playing field in terms of who gets these diseases and who doesn’t,” says Nicole Lurie, U.S. director of the Coalition for Epidemic Preparedness Innovations (CEPI), a foundation formed specifically to develop and improve access to vaccines for diseases that lack strong market demand. “But frankly, it was a really long road to get to that kind of equity.”
Setbacks through the 1990s led global health leaders to rethink their approach, and in 2000 Gavi was founded collaboratively by the WHO, UNICEF, the World Bank and the Gates Foundation. Thanks to Gavi, says Violaine Mitchell, director of immunization at the Gates Foundation, “now countries not only assume but demand that when a vaccine is introduced in the developed world, it’s also made available in the developing world.”
Gavi has vaccinated more than one billion children with a routine suite of shots and given a total of 1.8 billion immunizations to people of all ages through campaigns for illnesses such as measles in Ethiopia, Afghanistan and Somalia and yellow fever in Congo, averting more than 17 million deaths through 2022. Since Gavi was established, there has been a 70 percent reduction in deaths from vaccine-preventable diseases in children living in the lower-income countries the alliance supports, and mortality among children younger than five years in those countries has been halved. The pneumococcal and rotavirus vaccines have been particularly significant—pneumonia and diarrhea are among the top global killers of children under five.
But even those impressive numbers don’t fully capture the dramatic ways vaccines advance health equity. For example, epidemics of meningococcal meningitis were common in the “meningitis belt,” a stretch of 26 countries just south of the Sahara desert that has the highest rates of meningococcal disease in the world. Up to half of those infected die without treatment; even with treatment, one in 10 people dies. Since the development and distribution of a vaccine against meningitis A, this form of the disease has been nearly eliminated. The vaccine has not only saved lives but prevented long-term effects that meningitis survivors often suffer, including hearing loss, seizures, limb amputations or weakness, scarring, vision problems and cognitive difficulties.
Another example is the human papillomavirus (HPV) vaccine, which can prevent up to 90 percent of HPV-related cancers, including nearly all cervical cancer. Because high-income countries implemented cervical cancer screening programs decades ago, 94 percent of global deaths from cervical cancer in 2022 were in low- and middle-income countries. Gavi programs have vaccinated more than 16 million girls worldwide against HPV, and the organization aims to vaccinate 86 million by 2025. The physical benefits won’t be seen for years—it takes up to two decades for an HPV infection to develop into cancer—but the ripple effects of prevention go far beyond saving a single person’s life. A death from cervical cancer may mean loss of a family caretaker, loss of income and difficulty meeting children’s continuing health needs. “The tsunami effect of losing a mother to children, especially for those who are not economically stable, is devastating to a family,” O’Brien says. “Their lives are entirely dependent on the survival of that person.”
Vaccination can be a key entry point to additional health care. William Foege, a former director of the U.S. Centers for Disease Control and Prevention, who was instrumental in leading smallpox eradication and in setting up Gavi, called vaccines “the tugboat” for preventive care.
When health workers arrive to vaccinate children in a community, they can assess other children’s growth trajectories and nutritional issues, provide vitamin A supplements where there are deficiencies, distribute deworming tablets, monitor mosquito-borne diseases and check on additional needs. “If you manage to reach a child and give them a measles vaccine, then you may be able to give their mother maternal services,” Nguyen says. “It’s a perfect time to say: Are you sleeping under a bed net? Do you need a bed net? What are you doing for family planning?” Mitchell says. “All those conversations can come about because of the contact between the caregiver and the health worker that wouldn’t [otherwise] happen.”
In 1985 Rotary International launched its PolioPlus program, which used vaccination campaigns as an opening for other health interventions. “When Rotary and its partners added other things to improve the health systems of countries, it was a game changer,” says Stella Anyangwe, a Rotary International EndPolioNow coordinator and former WHO official. By strengthening laboratory systems, the cold-chain network of refrigerated storage necessary for transporting the vaccine, and overall disease surveillance, she says, improving systems for polio eradication “strengthened the health systems in general.” In short, Levine says, “immunization is an innovation that is pulling other innovations along.”
It can also free up valuable time and resources in health care. As infectious disease incidence falls, health workers and hospital beds become available for people with other conditions. This may already be happening with malaria. In Burkina Faso, about two out of every five visits to a health-care provider are for malaria, which historically accounts for more than 60 percent of the country’s hospitalizations. Similarly, malaria cases make up about half of hospitalizations in Cameroon; most of those patients are children under five who are eligible for the malaria vaccine. Although current malaria vaccines don’t prevent infection altogether, they reduce severe disease by 30 percent and all-cause mortality by 13 percent. Gavi began rolling out vaccination campaigns against malaria last year, providing 18 million doses to a dozen African countries, and malaria deaths have already begun falling. “You can imagine how much that’s going to free up capacity for health-care workers to focus on other [issues],” Nguyen says.
Vaccines help countries with fewer resources protect themselves from disease. Outbreaks disproportionately affect poorer areas: the 2014–2016 Ebola epidemic in West Africa, for example, devastated the region’s health-care infrastructure. Since the development of an Ebola vaccine in the late 2010s, subsequent outbreaks have remained comparatively small. And the current outbreak of mpox, which led the WHO to declare a global public health emergency in August, is being managed with vaccines that became available only in the past few years.
Gavi now supports stockpiles of outbreak-specific vaccines for cholera, yellow fever, meningococcal disease and Ebola so the countries most affected can focus their health-care resources on chronic disease, snakebites, cancer and HIV, among other conditions.
In late 2019, when a novel coronavirus detected in Wuhan, China, kicked off one of the largest, deadliest pandemics in a century, everyone looked to the same solution: a vaccine. COVID’s devastation hit poorer countries with less developed health-care systems particularly hard, and in wealthier countries people from underserved and low-income communities suffered higher rates of illness, death and economic hardship. It was clear that a COVID vaccine would be the most equitable solution.
The U.S. quickly directed $10 billion toward vaccine development, and dozens of other countries allocated what they could. The effort broke every record for the fastest vaccine development. The Chinese CDC released the sequence of SARS-CoV-2 on January 10, 2020, and just 11 months later, on December 8, 2020, the first COVID vaccine was administered outside of a clinical trial.
Officials at Gavi, UNICEF, WHO and CEPI quickly organized Covax, an international effort to accelerate COVID vaccine development and “to guarantee fair and equitable access for every country in the world,” according to the WHO. Covax delivered nearly two billion vaccines to more than 140 countries in the two years after the vaccines’ introduction, “by far the fastest, largest and most effective public health roll-out in history,” a Gavi spokesperson says. A 2022 study in the Lancet Infectious Diseases estimates that COVID vaccination worldwide prevented 19.8 million excess deaths, 7.4 million of those in Covax countries.
The challenges were steep and vaccine distribution contentious. “At no point did a richer country with access to vaccine doses choose to slow down its rollout to make doses available for people at higher risk in lower-income countries,” Levine says. “That’s vaccine nationalism, and it undermined the success of hardworking folks at Covax.”
Those problems have prompted a lot of reflection and a lot of new action. The organizations behind Covax have now set their sights on improving vaccine equity during future pandemics. Because Africa lacked vaccine access and had few manufacturing capabilities of its own, the new efforts are particularly focused on boosting the continent’s vaccine-manufacturing capabilities. The Africa CDC has partnered with other organizations to create the Partnerships for African Vaccine Manufacturing with a goal of making 60 percent of its needed vaccines by 2040. In June 2024 Gavi launched the African Vaccine Manufacturing Accelerator, a financing program developed with the Africa CDC and African Union to put up to $1.2 billion over the next decade toward building up the continent’s vaccine-manufacturing capacity.
In the almost 25 years since Gavi was launched, it has made substantial progress in advancing equity in vaccine manufacturing. In 2000 four of its five vaccine suppliers were in wealthy countries. Today most of its 20 or so suppliers are in developing countries. “It opened up a marketplace for large-scale, low-cost manufacturing in India, in Brazil, in China and in Indonesia,” says Berkley, former Gavi CEO.
It will still be immensely challenging to get vaccines into the arms and mouths of people who need them most. Health workers must find and immunize zero-dose children—children who have yet to receive vaccines of any kind, like the ones Laja sees in South Sudan. And low-income countries must acquire the financing and build the infrastructure to facilitate that process. Then Laja and her peers must educate people so fear does not become a barrier to access.
Workers such as Laja are part of the global workforce that the WHO, Gavi, UNICEF, the Gates Foundation, Rotary, and other organizations have trained to use vaccines against disease and health disparities. Earlier this year Laja completed training in preparation for South Sudan’s malaria-vaccine rollout. In 2022 there were almost 7,000 malaria deaths in South Sudan, and the disease is the top killer of young children in the country. The previous year South Sudan’s malaria fatalities accounted for more than 1.2 percent of the total worldwide.
Laja is eager to see the vaccines’ impact on her community and in the villages she visits, where parents will walk for miles from outlying areas to meet her. “There are very few things women and caretakers will walk hours and hours for, but vaccines are still one of them,” says Mitchell of the Gates Foundation. “People will literally drop everything to come and vaccinate their child.”
The journey toward health equity can, at times, feel endless. But it can also be exciting and inspiring. Scientific American asked some of the researchers, physicians, advocates, and others working on health equity what they are most hopeful about. Each had numerous concerns but also reasons for optimism. They pointed to progress in widening access to health care, making science more inclusive, and reducing the health burden of systemic racism and other biases. They are also emboldened by the energy and enthusiasm of their colleagues working to advance health equity.
“Any level of justice work has to be rooted in a context of hope, right?” says Aletha Maybank, chief health equity officer at the American Medical Association. “A hope and faith that we will all be able to have an experience of optimal health.”
Madhukar Pai
Chair, Epidemiology and Global Health, McGill University
Credit: Courtesy of Pai Madhu
My biggest source of hope is young people. It’s the youngest people who are shining a clear light on why climate change is devastating and why leaders are not acting on what has been obvious for many years. It’s the youngest people who are doing great work in the U.S. on gun control, even as they’re getting slaughtered in schools. It’s the young people who are alarmed about the rollback of reproductive rights in the U.S., in Afghanistan, you name it.
I feel like their moral clarity is the clearest because, unlike older people who already bought into something or were worried about their next paycheck or position or winning awards, young people are devastatingly clear in terms of what’s wrong. Their problem statements are spectacularly accurate and on point, and so they give me a huge amount of hope. That’s partly why I still teach global health to young people.
Just fanning their energy, their passion, might well be the biggest source of hope for all of humankind. But we need to go beyond that because although their diagnosis is perfect, their ability to act is limited. They’re not in power; they often are not voting. They’re usually given two minutes to speak at the front end of the meeting and shown out of the door while the adults are making big decisions. So how do we potentiate them to go beyond just sound bites or nice photo ops to action and give them empowered ways of doing things?
Seye Abimbola
Associate Professor, Health Systems, University of Sydney
Credit: University of Sydney
One of the things about which I’m hopeful is a growing confidence and restlessness and disquiet from global health professionals and academics from and in the Global South about how the field itself works and needs to change. Historically the field was premised on this idea that the West—or the Global North, as we refer to it today—has a right and a duty to impose itself on the rest of the world.
For example, if someone wanted to do a study in Nigeria and the people who are going to lead it come from London, they would rely on a lot of the infrastructure in Nigeria but disregard that the local collaborators know anything. Then they go home and write this paper and publish it in the BMJ or in the Lancet. Now, for me, what I think has changed, what I see changing more and more, is the pushback on that. That’s just the tip of the iceberg. But that physically measurable, countable phenomenon of partnership research sits on a whole bed of assumptions and normalized practices that we took from the colonial experience.
Rachel Hardeman
Director, Center for Antiracism Research for Health Equity, University of Minnesota School of Public Health
Credit: Chris Cooper/University of Minnesota School of Public Health
One of the things that gives me hope is the work that I’m doing, along with many other incredibly brilliant scholars across the country, around measuring racism. In my work and within our research center, we have to be able to make the invisible visible. Racism is so often passed off as this insidious thing that is baked into the system, and it’s so hard to identify, especially when it’s not an explicit interaction with someone.
In a lot of my work and in what I’m seeing across the country with other scholars—incredibly brilliant Black scholars in particular—is an investment and interest in figuring out how we leverage data to measure structural and other forms of racism and then how to use that to inform policy change. We’re coalescing around the need to understand that health policy and social policy go hand in hand. We can’t, for example, talk about historical redlining and racial covenants and birth outcomes in those communities without having the data, without understanding the history as well as what’s happening currently. And then using that to inform housing policy just as much as we might use that evidence to inform health policy.
Wafaa El-Sadr
Director, Global Health Initiative, Columbia University mailman school of public health
Credit: Hugh Siegel/ICAP at Columbia University
When I think back to what things looked like 25 years ago, compared with today, it’s night and day. Investments in health systems, largely driven by the HIV epidemic, have borne fruit in amazing ways. No services were available, or those that did exist were fractured. There were no resources; there was no access to medicines or lab tests. It’s just been an enormous transformation in only a couple of decades, so that gives me hope for the future.
More than 20 years ago I remember going to a clinic very far away from the capital city in one of the provinces in South Africa. There was nothing available for HIV testing or for treatment, and, I remember this vividly, this nurse very proudly opened a notebook that she had in a drawer in her very rickety desk and said, “I have a list of people here who need treatment.” And then she pulled out another sheet of paper, and she said, “Look at this. I have a certificate. I’ve been trained. I’m ready. I want to save my people.” And I remember walking away thinking, “This gives me hope. There are people who care about their communities. They’re ready, they’re willing.” And I’ll never forget that, and I’ll never forget the look on her face of “I can’t wait anymore.”
Barney Graham
Founding Director, David Satcher Global Health Equity Institute, Morehouse School of Medicine
Credit: Morehouse School of Medicine
Hopefulness comes from a faith and belief that things have a way of evolving toward the good. The moral arc of the universe bends toward the good. But it may take a long time. Helping to diversify the public health workforce through creating more opportunities and knowledge for students is a multigenerational process.
Four African American students did almost all the bench work that was needed to get the Moderna COVID vaccine into that first phase 1 trial in March 2020. We’re very proud of them for getting that whole vaccine program launched.
We must change the narrative of what people can do and what they are able to do and start asking, Who gets to be trained? Who gets to have the knowledge? Who gets to make the decisions? Who gets to decide what to make and where it goes? All those decisions happen at some level of leadership. If you diversify that leadership, you will have a better, more balanced opinion about how things should be done. That’s how you start moving toward equity.
Aletha Maybank
Chief Health Equity Officer, American Medical Association
Credit: American Medical Association
It’s helpful looking at progress. The past four years, since the public murder of George Floyd, there is now the ability to mention racism where you couldn’t before. Prior to the public murder of George Floyd, folks would never have expected the AMA to make a statement about racism being a public health threat. And then the AMA’s House of Delegates passed a policy that really reaffirms ridding medicine of medical essentialism and ridding medicine of the use of race as a proxy for biology. That has been aligned with a movement around getting rid of racist algorithms, clinical algorithms. That would have never started without this national and collective movement to name racism and the exposure of inequities during COVID. That response and that collective response do provide hope.