Announcing a new publication for Acta Materia Medica journal. G protein-coupled receptors (GPCRs) are important, potential drug targets for the treatment of metabolic disorders, such as obesity. GPCRs crosstalk with several transducers, including heterotrimeric G proteins, GPCR kinases (GRKs), and β-arrestins.
GPCR-biased agonism has raised the potential of novel drug development to preferentially activate therapeutic signaling pathways over pathways that lead to unwanted side effects. The obesity epidemic and its metabolic complications continue to be a major global public health threat but effective treatments are limited. The accelerated development of structural techniques, like X-ray crystallography and cryo-electron microscopy, has paved the way to understanding how biased agonism measured at GPCRs results in specific downstream physiologic responses.
The authors of this article summarize well-validated GPCR targets and outline several new and promising receptors for obesity treatment. The significance of deciphering the role of GPCRs in obesity pathology and biased signaling for drug development are highlighted.
Source:
Journal reference:
Shen, S., et al. (2024) G protein-coupled receptor-biased signaling: potential drug discovery to facilitate treatment of metabolic diseases. Acta Materia Medica. doi.org/10.15212/AMM-2023-0041.
In a recent study published in the journal Nature Metabolism, a team of scientists investigated whether modulation of the gut microbiome using dietary fiber supplementation in the form of resistant starch could help with insulin resistance and weight loss and offer a potential treatment avenue for metabolic disorders.
Obesity has been classified as a global epidemic, with substantial research being conducted on strategies to reduce weight and prevent obesity. It contributes significantly to the global mortality rates by increasing the risk of metabolic diseases such as diabetes, as well as cardiovascular disease risk. Weight management and effective weight loss can lower the risk of these diseases.
Increasing evidence indicates that the gut microbiome plays a pivotal role in the regulation of human physiology and development of various diseases. Gut microbiome composition and diversity are intricately linked to the metabolism of glucose and fat and inflammation.
Furthermore, while fecal microbiome transplantation has been used to establish healthy gut microbiome communities, the procedure has not yielded effective or long-term results. However, diet can be used to modulate the gut microbiome, and dietary interventions, either alone or in conjunction with fecal microbiome transplantation, could potentially improve the clinical outcomes.
About the study
In the present study, the team conducted a randomized, crossover clinical trial involving overweight individuals to determine whether dietary supplementation with resistant starch positively impacted obesity and metabolic phenotypes. They also conducted metagenomic and metabolomic analyses to understand how the resistant starch affected the composition of the gut microbiome and its function.
Furthermore, they studied antibiotic-treated mice that had received gut microbiomes from human donors that had already been modified through resistant starch supplementation to understand how gut microbiomes modified through supplementation with resistant starch influence glucose metabolism and adiposity. The metabolomic advantages offered by the gut microbiome modified through resistant starch supplements were also explored.
Resistant starch cannot be broken down by the amylase enzymes produced in humans, functioning as a dietary fiber. During digestion, resistant starch does not get broken down in the stomach or small intestine but moves into the large intestine or colon, where the gut microbiome ferments this dietary fiber. Rodent model studies have shown a decrease in body fat and better metabolic outcomes when the carbohydrate portion of their diet consists mainly of resistant starch.
The present clinical trial included participants with excess body weight who did not have any chronic disorders, were not using any probiotics or antibiotics, and were not undergoing any treatments that would impact their glucose metabolism. The participants were randomly assigned to the treatment or control group, with the treatment group receiving resistant starch in the form of high-amylose maize and the control group receiving amylopectin with no resistant starch.
The starch was provided in sachets in powdered form, and all the participants in the treatment and control groups consumed one packet of the appropriate starch twice a day before a balanced, isoenergetic meal that was provided thrice a day. Since this was a crossover clinical trial, all the participants underwent two eight-week-long interventions, one for the resistant starch treatment and the other for the control treatment.
Results
The results showed that supplementation with resistant starch helped achieve a mean weight loss of about 2.8 kg and improved insulin resistance in overweight participants. The study also found that the beneficial effects of resistant starch supplementation were associated largely with gut microbiome composition changes.
The bacterium Bifidobacterium adolescentis was found to be associated with resistant starch supplementation in humans, and the monocolonization of mice with this bacterium protected them from diet-induced obesity. Resistance starch impacted lipid and fat metabolism by reducing inflammation, restoring the intestinal barrier, and altering the bile acid profile.
The gut microbiota impacts the host physiology through signaling metabolites, of which bile acids play a significant role. Secondary bile acids, such as glycodesoxycholic acid, deoxycholic acid, glycocholic acid, and taurodeoxycholic acid, are important in improving insulin sensitivity and ameliorating hepatic steatosis. The enzyme bile salt hydrolase carries out the deconjugation of secondary bile acids.
The study found that resistant starch supplementation decreased the production of bile salt hydrolase and increased the levels of secondary bile acids. The results were reciprocated in the mice after they were monocolonized with B. adolescentis from humans who underwent resistant starch supplementation.
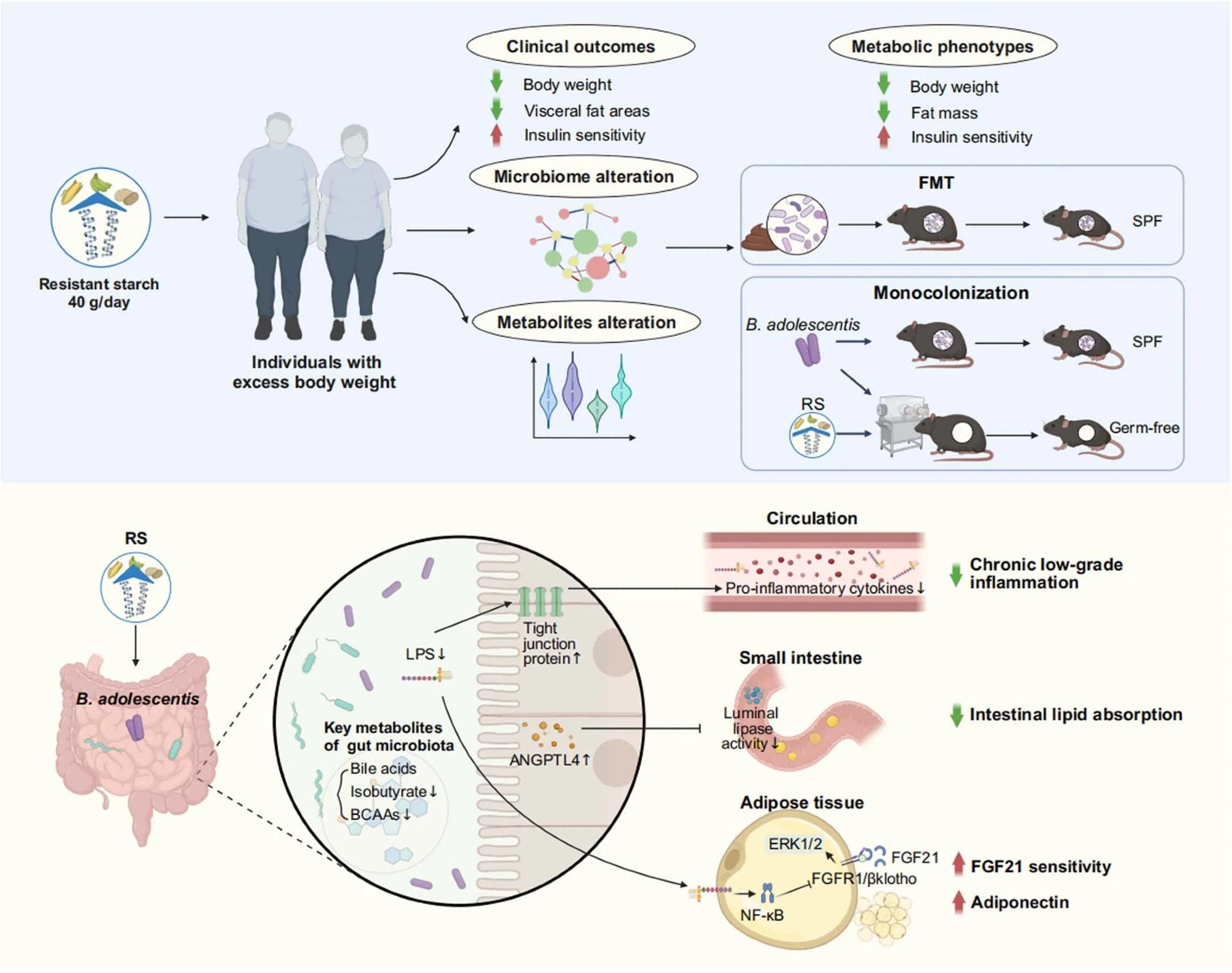
Resistant starch (RS, 40 g d-1) accompanied with isoenergetic and balanced diets led to an obvious reduction in body weight and improvement of insulin sensitivity, as well as alteration in metagenomics and metabolomics. Faecal microbiota transplantation (FMT) showed benefits of RS were associated with the reshaped gut microbiota composition. Monocolonization of mice with B. adolescentis, which was closely correlated with the benefits of RS in human protected mice from diet-induced obesity. Mechanistically, the RS-induced changes in the gut microbiota influenced metabolites of gut microbiome, reduced chronic low-grade inflammation by improving intestinal integrity, inhibited lipid absorption by modulating angiopoietin-like 4 (ANGPTL4), and improved the sensitivity of fibroblast growth factor 21 (FGF21) in adipose tissue. SPF, specific-pathogen-free; LPS, lipopolysaccharide; BCAAs, branched-chain amino acids; Erk1/2, extracellular signal-regulated kinase 1/2; FGFR1, fibroblast growth factor receptor 1. Created with BioRender.com.
Conclusions
To summarize, the study found that supplementation with resistant starch can facilitate weight loss by increasing the abundance of B. adolescentis in the gut microbiome. It can also help improve insulin sensitivity through gut microbiome-induced changes in the levels of secondary bile acids and lowering of inflammation.
Journal reference:
Li, H., Zhang, L., Li, J., Wu, Q., Qian, L., He, J., Ni, Y., KovatchevaDatchary, P., Yuan, R., Liu, S., Shen, L., Zhang, M., Sheng, B., Li, P., Kang, K., Wu, L., Fang, Q., Long, X., Wang, X., & Li, Y. (2024). Resistant starch intake facilitates weight loss in humans by reshaping the gut microbiota. Nature Metabolism. DOI: 10.1038/s4225502400988y, https://www.nature.com/articles/s42255-024-00988-y
In a recent study published in the British Medical Journal, researchers investigated the link between non-alcoholic fatty liver disease (NAFLD) in individuals with type 2 diabetes mellitus (T2DM) and all-cause death and cardiovascular disease. They found that individuals with NAFLD and T2DM show an increased risk of cardiovascular disease (CVD) and all-cause death.
The prevalence of NAFLD is on the rise globally and is often associated with metabolic disorders involving insulin resistance. It poses a significant health concern due to its potential to lead to liver complications and CVD, which is a leading cause of mortality, especially among NAFLD patients.
T2DM is a major risk factor for CVD and is closely linked to higher NAFLD prevalence and severity. The complex relationship between NAFLD and T2DM suggests a synergistic effect on cardiovascular risk, with a substantial proportion of T2DM patients also having NAFLD. However, studies examining their association with CVD have yielded mixed results. While some found no correlation, others demonstrated a doubled risk of CVD in T2DM patients with NAFLD compared to those without. Additionally, previous studies were limited by their cross-sectional designs and small sample sizes.
To address this gap, researchers in the present study aimed to assess the risk of CVD and all-cause mortality associated with NAFLD in T2DM patients using a large-scale, population-based longitudinal approach.
About the study
This nationwide cohort study utilized data from the National Health Information Database linked t the National Health Screening Program. The exclusion criteria were age ≤ 20 years, consumption of ≥30 g/day alcohol, missing data, or a history of type 1 diabetes mellitus, chronic hepatitis B, and C, liver cirrhosis, hepatocellular carcinoma, or CVD. Additionally, patients who developed CVD within one year were also excluded.
A total of 7,796,763 participants were selected, and the endpoint was the occurrence of all-cause death, CVD, or until 31 December 2018. CVD included myocardial infarction or ischemic stroke, confirmed through hospital admissions with corresponding claims for brain magnetic resonance imaging or computed tomography. The patients were followed-up for a median of 8.13 years.
Data on anthropometric measurements and laboratory parameters were collected. Blood pressure was measured in a seated position, and fasting venous blood samples were taken to assess various parameters, including glucose, liver enzymes, lipid profile, and creatinine levels. Additionally, the estimated glomerular filtration rate was determined.
Information on lifestyle factors such as smoking, alcohol consumption, regular exercise, and socioeconomic status was obtained through a standardized self-assessment questionnaire. Statistical methods included Cox proportional hazards models adjusted for various factors, Kaplan-Meier survival curves, and subgroup analyses.
Results and discussion
Among the participants, 6.49% of the participants had T2DM. Grade 1 and 2 NAFLD were found in 22.04% and 11.11% of participants, respectively. A higher proportion of T2DM patients had grade 2 NAFLD (26.73%) and grade 1 NAFLD (34.06%) compared to those without T2DM. Among participants with T2DM, 6.77% had CVD, and about 8.38% of participants died. In contrast, among those without T2DM, 2.24% had CVD, and about 2.71% of participants died.
Incidence rates for CVD, myocardial infarction, ischemic stroke, and all-cause mortality increased with the severity of NAFLD and were higher in patients with T2DM than in those without. Hazard ratios for these outcomes were also higher with grade 1 and grade 2 NAFLD compared to no NAFLD, regardless of T2DM status. Moreover, the five-year absolute risk for these outcomes increased with NAFLD severity, particularly in patients with T2DM. Risk differences for CVD, myocardial infarction, ischemic stroke, and all-cause death were higher between no NAFLD and grade 2 NAFLD than between no NAFLD and grade 1 NAFLD. Additionally, these risk differences were higher in patients with T2DM compared to those without T2DM.
NAFLD was linked to an increased risk of cardiovascular disease, myocardial infarction, ischemic stroke, and all-cause death in both T2DM and non-T2DM patients (p<0.001). Among NAFLD patients, those with grade 2 NAFLD exhibited the highest risk, followed by grade 1 NAFLD.
Further, the incidence rates of CVD, myocardial infarction, ischemic stroke, and all-cause death increased sequentially from no NAFLD to grade 1 NAFLD and to grade 2 NAFLD across all age groups, with higher rates observed in T2DM patients.
The study’s limitations include the use of the fatty liver index for NAFLD definition, lack of assessment of glycated hemoglobin variability and changes in diabetes drugs, limited generalizability to other ethnicities, and the inability to evaluate hepatic fibrosis.
Conclusion
In conclusion, patients with T2DM and even mild NAFLD have a higher risk of cardiovascular disease and all-cause death. The risk gap between no NAFLD and grade 1 or grade 2 NAFLD is more significant in T2DM patients than in those without. The findings emphasize the need for NAFLD screening and prevention in T2DM patients to reduce subsequent cardiovascular risk and mortality.
A study led by the University of Barcelona and the Biomedical Research Networking Center in Diabetes and Associated Metabolic Disorders (CIBERDEM) reveals how a new mechanism could improve the efficiency of currently available treatments for diabetes. The study, carried out on mice and cell cultures, may open up new ways of approaching metabolic diseases that are a global health problem.
The study, published in the journal Metabolism, focuses on the GDF15 protein, a factor that is expressed at high levels in many diseases, such as heart failure, cancer and fatty liver disease. Obese patients also have elevated levels of this protein, but its function is altered and those affected may develop resistance to GDF15 — that is, a reduction in the effectiveness of its activity.
The study is led by Professor Manuel Vázquez-Carrera, from the Faculty of Pharmacy and Food Sciences of the UB, the Institute of Biomedicine of the UB (IBUB), the Sant Joan de Déu Research Institute (IRSJD) and CIBERDEM. The study also highlights the participation of researchers Patricia Rada and ángela María Valverde, also collaborators at CIBERDEM, the Spanish National Research Council (CSIC) and the Autonomous University of Madrid (UAM). The work has the collaboration of Professor Walter Wahli of the University of Lausanne (Switzerland), among other experts.
New alternatives to reduce glucose synthesis in the liver
Our study reveals that GDF15 inhibits glucose synthesis in the liver. This pathway plays a decisive role in the generation of hyperglycemia (increased blood glucose levels) in patients with type 2 diabetes mellitus.”
Professor Manuel Vázquez-Carrera
“The action of the protein would also help reduce the presence of liver fibrosis, a condition associated with increased mortality in patients with fatty liver disease”, the researcher notes.
The study reveals that mice deficient in GDF15 have glucose intolerance and low levels of AMPK protein in the liver, which is a sensor of energy metabolism in the cell against type 2 diabetes.
Moreover, increased glucose synthesis in the liver (hepatic gluconeogenesis) was also detected in these study models, as well as increased liver fibrosis.
All indications are that all the described alterations were triggered by increased hepatic levels of transforming growth factor-beta 1 (TGF-β1) and an SMAD3mediator protein, which are the main inducers of liver fibrosis. Thus, treatment with recombinant CDF15 can activate AMPK and decrease levels of active SMAD3 in mouse liver and in primary hepatocyte cultures.
“In conclusion, the results indicate that GDF15 activates AMPK protein and inhibits hepatic gluconeogenesis and fibrosis through the reduction of the TGF-β1/SMAD3 pathway”, says Vázquez-Carrera.
“These results suggest that modulation of GDF15 levels could be useful to improve the effectiveness of current anti-diabetic treatments, as hepatic gluconeogenesis is key in hyperglycaemia in patients with type 2 diabetes mellitus, and serum TGF-β1 levels are also increased in these patients”, concludes the researcher.
Source:
Journal reference:
Jurado-Aguilar, J., et al. (2024). GDF15 activates AMPK and inhibits gluconeogenesis and fibrosis in the liver by attenuating the TGF-β1/SMAD3 pathway. Metabolism. doi.org/10.1016/j.metabol.2023.155772.
Males born to obese women are more likely to be overweight at birth and develop metabolic complications in later life, including liver disease and diabetes.
Image Credit: University of South Australia
The way that male sex hormones activate pathways in the developing liver is partly to blame.
That’s the finding from a new study led by University of South Australia (UniSA) researchers looking at the impact of maternal obesity on fetal liver androgen signalling.
Male fetuses of obese pregnant women have different signals that are activated by male sex hormones in the liver, which encourages them to prioritize growth at the expense of their health.
UniSA researcher Dr Ashley Meakin says androgens give men their male characteristics and are crucial in their development, but if there are too many, male fetuses grow too large, causing not only problems at birth, but impacting liver function as an adult.
Female fetuses exposed to excess testosterone from an obese pregnancy are wired to switch off the androgen pathway in the liver, restricting their growth and lowering the risks of metabolic disorders in adulthood.
We know there are sex differences in metabolic disorders in later life in response to maternal obesity. Men are more prone to non-alcohol fatty liver diseases and diabetes as an adult if their mother is obese during pregnancy and their birth weight is above 4 kg (9 lb 15 oz). They are genetically wired to prioritize androgens because it supports the development of male characteristics – including size – but too much androgen is bad.”
Dr Ashley Meakin, UniSA Researcher
Study lead author Professor Janna Morrison, Head of the Early Origins of Adult Health Research Group at UniSA, says it’s a fine balance for women getting the right nutrition in pregnancy to ensure optimal conditions for their unborn child to flourish.
“There are also risks for offspring being malnourished during pregnancy,” she says. “If you are too little, too big, born too early, or a male, you are more vulnerable to negative outcomes later in life. You need the Goldilocks pregnancy: you must be the right size, born at the right time.”
Prof Morrison says unless society changes its approach to nutrition, it will be an uphill battle to reduce obesity and associated health issues, from the womb into adulthood.
“As a society, we urgently need to address obesity. If children were taught early on about the importance of healthy eating, it would carry through into adulthood, including during pregnancy, where the right nutrition is so important.”
Dr Meakin says in the intervening period, supplements that address nutritional imbalances in pregnancy could provide the fetus with the best chance of optimal development.
The liver androgen signalling study, recently published in Life Sciences, is among a series of studies by Prof Morrison and colleagues that investigates the impact of maternal under- and over-nutrition on the placenta, heart, lung, and liver.
Males born to obese women at higher risk of liver diseases as adults
Meakin, A. S., et al. (2024). Maternal obesity impacts fetal liver androgen signalling in a sex-specific manner. Life Sciences. doi.org/10.1016/j.lfs.2023.122344.