Rice University engineers have developed the smallest implantable brain stimulator demonstrated in a human patient. Thanks to pioneering magnetoelectric power transfer technology, the pea-sized device developed in the Rice lab of Jacob Robinson in collaboration with Motif Neurotech and clinicians Dr. Sameer Sheth and Dr. Sunil Sheth can be powered wirelessly via an external transmitter and used to stimulate the brain through the dura ⎯ the protective membrane attached to the bottom of the skull.
The device, known as the Digitally programmable Over-brain Therapeutic (DOT), could revolutionize treatment for drug-resistant depression and other psychiatric or neurological disorders by providing a therapeutic alternative that offers greater patient autonomy and accessibility than current neurostimulation-based therapies and is less invasive than other brain-computer interfaces (BCIs).
In this paper we show that our device, the size of a pea, can activate the motor cortex, which results in the patient moving their hand. In the future, we can place the implant above other parts of the brain, like the prefrontal cortex, where we expect to improve executive functioning in people with depression or other disorders.”
Jacob Robinson, professor of electrical and computer engineering and of bioengineering, Rice University
Existing implantable technologies for brain stimulation are powered by relatively large batteries that need to be placed under the skin elsewhere in the body and connected to the stimulating device via long wires. Such design limitations require more surgery and subject the individual to a greater burden of hardware implantation, risks of wire breakage or failure and the need for future battery replacement surgeries.
“We eliminated the need for a battery by wirelessly powering the device using an external transmitter,” explained Joshua Woods, an electrical engineering graduate student in the Robinson lab and lead author on the study published in Science Advances. Amanda Singer, a former graduate student in Rice’s applied physics program who is now at Motif Neurotech, is also a lead author.
The technology relies on a material that converts magnetic fields into electrical pulses. This conversion process is very efficient at small scales and has good misalignment tolerance, meaning it does not require complex or minute maneuvering to activate and control. The device has a width of 9 millimeters and can deliver 14.5 volts of stimulation.
“Our implant gets all of its energy through this magnetoelectric effect,” said Robinson, who is founder and CEO of Motif, a startup working to bring the device to market. “The physics of that power transfer makes this much more efficient than any other wireless power transfer technologies under these conditions.”
Motif is one of several neurotech companies that are probing the potential of BCIs to revolutionize treatments for neurological disorders.
“Neurostimulation is key to enabling therapies in the mental health space where drug side effects and a lack of efficacy leave many people without adequate treatment options,” Robinson said.
The researchers tested the device temporarily in a human patient, using it to stimulate the motor cortex ⎯ the part of the brain responsible for movement ⎯ and generating a hand movement response. They next showed the device interfaces with the brain stably for a 30-day duration in pigs.
“This has not been done before because the quality and strength of the signal needed to stimulate the brain through the dura were previously impossible with wireless power transfer for implants this small,” Woods said.
Robinson envisions the technology being used from the comfort of one’s home. A physician would prescribe the treatment and provide guidelines for using the device, but patients would retain complete control over how the treatment is administered.
“Back home, the patient would put on their hat or wearable to power and communicate with the implant, push ‘go’ on their iPhone or their smartwatch and then the electrical stimulation from that implant would activate a neuronal network inside the brain,” Robinson said.
Implantation would require a minimally invasive 30-minute procedure that would place the device in the bone over the brain. Both the implant and the incision would be virtually invisible, and the patient would go home the same day.
“When you think about a pacemaker, it’s a very routine part of cardiac care,” said Sheth, professor and vice-chair of research, McNair Scholar and Cullen Foundation Endowed Chair of Neurosurgery at the Baylor College of Medicine. “In neurological and psychiatric disorders, the equivalent is deep brain stimulation (DBS), which sounds scary and invasive. DBS is actually quite a safe procedure, but it’s still brain surgery, and its perceived risk will place a very low ceiling on the number of people who are willing to accept it and may benefit from it. Here’s where technologies like this come in. A 30-minute minor procedure that is little more than skin surgery, done in an outpatient surgery center, is much more likely to be tolerated than DBS. So if we can show that it is about as effective as more invasive alternatives, this therapy will likely make a much larger impact on mental health.”
For some conditions, epilepsy for example, the device may need to be on permanently or most of the time, but for disorders such as depression and OCD, a regimen of just a few minutes of stimulation per day could suffice to bring about the desired changes in the functioning of the targeted neuronal network.
In terms of next steps, Robinson said that on the research side he is “really interested in the idea of creating networks of implants and creating implants that can stimulate and record, so that they can provide adaptive personalized therapies based on your own brain signatures.” From the therapeutic development standpoint, Motif Neurotech is in the process of seeking FDA approval for a long-term clinical trial in humans. Patients and caregivers can sign up on the Motif Neurotech website to learn when and where these trials will begin.
The work was supported in part by The Robert and Janice McNair Foundation, the McNair Medical Institute, DARPA and the National Science Foundation.
Source:
Journal reference:
Woods, J. E., et al. (2024) Miniature battery-free epidural cortical stimulators. Science Advances.doi.org/10.1126/sciadv.adn0858.
Re-perfusing the lungs of an organ donor after the heart has irreversibly stopped beating with a technique called normothermic regional perfusion (TA-NRP) could potentially increase the number of patients receiving lung transplants, according to researchers at the Annual Meeting and Scientific Sessions of the International Society for Heart and Lung Transplantation (ISHLT) in Prague.
TA-NRP uses a machine to pass blood through a donor’s abdomen and chest after the heart has irreversibly stopped beating (called donation after circulatory death, or DCD). Thirty to forty minutes of perfusing blood to these areas reanimates the heart and ventilates the lungs.
Pedro Catarino, MD, director of Aortic Surgery at Cedars-Sinai Medical Center in Los Angeles, said techniques like TA-NRP will help get more of the available donor lungs to patients on the waiting list. Worldwide, the overall utilization of available donor lungs is only 20 percent.
The utilization of donor lungs is generally quite poor. For every five organ donors, we only use one set of lungs. It’s even worse for DCD donors, only four to six percent in the US. The great majority of DCD donors are not giving their lungs.”
Pedro Catarino, MD, Director of Aortic Surgery at Cedars-Sinai Medical Center
Dr. Catarino presented data showing that the retrieval rate for DCD lungs has increased to about 15 percent with the utilization of TA-NRP. However, some lung experts harbor concerns that lungs are injured during the in situ perfusion process.
“TA-NRP is technically possible, and some surgeons have successfully used it to retrieve both the heart and lungs from DCD donors,” said Shaf Keshavjee, MD, MSc, FRCSC, FACS, director of the Toronto Lung Transplant Program. “However, when TA-NRP was introduced in the US, the incidence of lung retrieval decreased.
“I think NRP could save more hearts, kidneys, livers, and lungs,” said Dr. Keshavjee. “But we need to standardize our technique because there are too many examples of good donor lungs damaged by TA-NRP.”
TA-NRP is currently only being used in the US and Spain. In Canada, DCD donor lungs are removed from the body and perfused outside the body (ex vivo) in a machine. Machine perfusion, which gives the surgical team control over the fluids used to perfuse the lungs, has been highly successful for the Toronto Lung Transplant Program.
“We have the largest lung transplant program in the world,” said Dr. Keshavjee. “We use 40 percent of DCD lungs, whereas the US uses only four percent.”
Unlike machine perfusion, which is not readily available worldwide, Dr. Catarino said that TA-NRP is a technique that anyone can use.
“Using TA-NRP, we’re also to measure the oxygen transfer in the lungs, which is a very good indicator of the quality of the donor’s lungs,” he said. “Being able to perform this functional assessment is one of its great benefits.”
Dr. Catarino said there is data that suggests outcomes following TA-NRP for DCD lungs are very good.
“TA-NRP is a way to get more lungs to patients who need them,” he said. “DCD was 32 percent of overall organ donors in the US in 2022, and the trajectory is going upward.”
The ISHLT has launched a task force to produce a statement that summarizes the best available evidence and practice for NRP, including outlining issues, concerns, and areas for future research.
Women are at higher risk of death when undergoing heart bypass surgery than men. Researchers at Weill Cornell Medicine have determined that this disparity is mediated, to a large extent, by intraoperative anemia-;the loss of red blood cells during surgery. The study, published on March 5, in the Journal of the American College of Cardiology, suggests that strategies for minimizing anemia that occurs during this procedure could lead to better outcomes for women with cardiovascular disease.
This study set out to discover why women are less likely to survive coronary artery bypass grafting, a surgical procedure for restoring blood flow to the heart. The team, led by senior author Dr. Mario Gaudino, the Stephen and Suzanne Weiss Professor in Cardiothoracic Surgery at Weill Cornell Medicine, analyzed information obtained from the Society of Thoracic Surgeons Adult Cardiac Surgery Database on more than one million patients. Dr. Lamia Harik, fellow in Cardiothoracic Surgery Research at Weill Cornell Medicine, was first author on the paper.
They examined patient demographics (such as age and ethnicity), risk factors (including disease severity, previous heart attacks and the co-occurrence of other health conditions) and surgical data (including the time spent on the bypass machine and the volume of the components of blood, such as red blood cells).
Crunching the numbers, Dr. Gaudino and his team previously confirmed that women had a higher mortality associated with the procedure than men: 2.8 percent versus 1.7 percent, a nearly 50 percent difference. Now, using sophisticated statistical analyses to assess all the possible variables, the researchers found that a substantial portion of this enhanced risk-;38 percent-;could be attributed to severe intraoperative anemia. This depletion of red blood cells is an inevitable side effect of using blood-diluting fluids to prime the heart-lung bypass machine that takes over the job of pumping blood throughout the body during surgery. Women may be even more susceptible to the effects of intraoperative anemia because they tend to arrive in surgery with lower red blood cell counts and have smaller body size compared to their male counterparts.
The study does not establish that intraoperative anemia is causing greater female mortality, but the two factors are associated. It suggests that clinicians and researchers should consider interventions to prevent or minimize severe intraoperative anemia, which can lead to dangerously reduced oxygen delivery to the body’s tissues, including the heart.
Using heart-lung bypass machines with shorter circuits, for example, would limit the volume of blood-diluting solution needed to run the pump. Randomized trials to assess whether methods for curtailing anemia could improve outcomes for women undergoing heart bypass surgery are “urgently needed,” wrote Dr. Gaudino, who is also a cardiovascular surgeon at NewYork-Presbyterian/Weill Cornell Medical Center.
This research was supported in part by the National Heart, Lung, and Blood Institute grant T32 HL160520-01A1, the National Institutes of Health, the Canadian Health and Research Institutes, and the Starr Foundation.
Source:
Journal reference:
Harik, L., et al. (2024). Intraoperative Anemia Mediates Sex Disparity in Operative Mortality After Coronary Artery Bypass Grafting. Journal of the American College of Cardiology. doi.org/10.1016/j.jacc.2023.12.032.
Severe sepsis from bacterial or viral infections can be life-threatening and even people recovering from severe sepsis may experience long-lasting effects on the immune system, making them more susceptible to recurrent infections. The causes for this sepsis-induced immune suppression are not well understood and lack an effective treatment. To better understand the cause, Katherine MacNamara and colleagues from Albany Medical College, USA, analyzed the blood stem cells of mice with prior sepsis and their results were recently published in the journal Stem Cell Reports.
During acute infection, blood stem cells in the bone marrow are activated by signaling molecules called inflammatory cytokines, which make them divide and migrate to the blood stream to generate large quantities of immune cells outside the bone marrow. Once infection is eliminated, cytokine levels return to baseline and blood stem cell activation and immune cell production stops.
To understand how this process gets dysregulated after severe sepsis resolves, the researchers analyzed the blood stem cells of mice and found them to be fully recovered and functional in the bone marrow of mice 20 days after sepsis. However, upon a second round of inflammatory stimulation, using the stem cell mobilizing agent G-CSF, the blood stem cells of sepsis survivors did not undergo a new round of activation and mobilization as did those in mice without prior sepsis.
Consequently, immune cells were not efficiently produced in those mice with prior sepsis. These observations could explain why following sepsis, patients are unable to efficiently combat new infections and why giving inflammatory cytokines and G-CSF specifically to sepsis patients had no effect against secondary infections in previous clinical trials. This knowledge may help to identify new treatments for patients with post-sepsis immune suppression.
Biswas, N., et al. (2024) Survivors of polymicrobial sepsis are refractory to G-CSF-induced emergency myelopoiesis and hematopoietic stem and progenitor cell mobilization. Stem Cell Reports. doi.org/10.1016/j.stemcr.2024.03.007.
While Obstructive Sleep Apnea (OSA) affects about five percent of the general pediatric population, 80 percent of children with Down syndrome experience OSA. Continual OSA results in poor health, including disruptions to cognitive development and functioning, leading physician-researchers from Mass General Brigham to investigate better methods to treat these patients as early as possible to maximize their health outcomes.
In a new case study published April 11 in Pediatrics, they report on a 4-year-old boy with Down syndrome and OSA who underwent a procedure to implant a hypoglossal nerve stimulation device, and experienced improvements thereafter.
Currently, adenoidectomies and tonsillectomies are among first-line treatments for pediatric OSA, however they are not always effective for children with Down syndrome because OSA can recur. Additionally, continuous positive airway pressure (CPAP) treatment, which streams compressed air into airways during sleep, is often not tolerated by children with Down syndrome due to sensory sensitivities.
The hypoglossal nerve stimulation device by Inspire has been an option increasingly used to treat OSA in adults since its 2014 FDA-approval. The device detects when the airway is blocked and sends an electrical pulse to the hypoglossal nerve that controls the tongue, causing it to move forward in the mouth, thereby opening the airway. Positive treatment data in adults first led lead study author Christopher Hartnick, MD, director of Pediatric Otolaryngology at Mass Eye and Ear, to wonder whether the treatment may help his patients with Down syndrome whose lives were impacted by OSA. With Mass General Brigham colleague Brian Skotko, MD, MPP, the Emma Campbell Endowed Chair on Down Syndrome at Massachusetts General Hospital, they organized a clinical trial looking at the safety and effectiveness of the procedure in children between the ages of 10 and 22 with Down syndrome. Results of a 42-patient trial showing the benefits and safety of the procedure were published in 2022, leading to FDA approval for the device for adolescents with Down syndrome over the age of 13 nearly a year later.
These results spurred the researchers to examine whether the procedure could benefit younger children who are impacted by the physical and neurocognitive effects of OSA during pivotal developmental years.
Hartnick and Skotko identified a patient candidate, 4-year-old Theodore “Theo” Scott of Knoxville, Tenn., who had been on CPAP therapy since he was 1 year old.
After Hartnick and his team had extensive discussions about potential risks with colleagues in other medical specialties and Theo’s parents, Rachel and Andrew Scott, a surgery took place in May 2023. The surgery was successful without complications, and the procedure was modified to allow for Theo’s continued growth.
After one month, Theo experienced an improvement in sleep, and his obstructive apnea-hypopnea index (a measure of apnea severity) decreased by 40 percent. Additional follow-up care will take place for Theo to monitor effects of the procedure on neurocognition and surveillance of the device as he grows.
“The most significant change we have seen is the amount of sleep Theo is now getting, routinely over 10 hours a night versus what we experienced with CPAP where he would pull his mask off up to fifteen times a night. Theo sleeping through the night has also benefitted us as parents since we would need to get up and assist him, and we could each feel the toll poor sleep was taking on our health,” Rachel and Andrew Scott said in a statement. “We have also noticed Theo wakes up more easily in the morning and has a longer attention span than before the surgery, and his language development has accelerated from one-word statements to multiple word sentences. This procedure has absolutely been a game-changing intervention in Theo’s life and in our family’s.”
Hartnick and Skotko are currently leading an NIH-sponsored 4-year trial examining the impact of upper airway stimulation on neurocognition and language in young patients with Down syndrome.
Children with Down syndrome are disproportionally affected by obstructive sleep apnea and often don’t benefit from traditional interventions, and research shows this impacts their cognitive development and IQ scores. The potential long-term impact on neurocognition was a major driver of our team and the family’s shared decision-making to pursue this treatment, and this case suggests it may be a possible option for some families.”
Christopher Hartnick, MD, Director of Pediatric Otolaryngology at Mass Eye and Ear
“In our Down Syndrome Program, I see first-hand how frustrated families become when their child with Down syndrome runs out of options to treat significant sleep apnea,” said Skotko. “Theo now opens up a new frontier for research and potential clinical care.”
Source:
Journal reference:
Wasserman, I., et al. (2024) Hypoglossal Nerve Stimulation for Obstructive Sleep Apnea in a Young Child With Down Syndrome. Pediatrics. doi.org/10.1542/peds.2023-063330.
Prediabetes is defined as glycated hemoglobin levels between 5.7-6.5% and fasting blood glucose levels between 100-126 mg/dL. Prediabetes significantly increases the mortality risks and burden on the healthcare system; therefore, several interventions have been designed to maintain healthy glucose levels.
For example, lifestyle changes, bariatric surgery, and medications are commonly used to prevent the progression of prediabetes to diabetes. Despite these interventions, a recent American Diabetes Association report indicated that most prediabetic patients eventually develop diabetes. Therefore, it is imperative to develop more effective interventions to prevent or reverse the prediabetic condition.
The gut microbiome and diabetes
The gut microbiome plays a vital role in regulating lipid and glucose metabolism, as gut microbial dysbiosis leads to the development of many diseases. For example, intestinal bacterial composition and abundance changes influence intestinal permeability, which induces insulin resistance and the introduction of bacterial lipopolysaccharides into the bloodstream.
Gut microbial dysbiosis is directly associated with increased gut permeability, which promotes low-grade systemic inflammation. This condition is a key contributor to metabolic syndrome and various chronic diseases, such as type 2 diabetes.
Considering these observations, it is important to understand the mechanism by which intestinal bacteria alterations influence the development of diabetes. This information could ultimately support the development of novel approaches to prevent the progression of prediabetes to diabetes.
Diet, drugs, and age play an important role in altering the gut microbiota. Although several studies have established differential intestinal bacteria between diabetic and healthy individuals, few studies have assessed intestinal bacteria composition in prediabetic patients and its impact on the physiological mechanisms of this health condition.
About the study
The current study compared gut microbial composition between prediabetic patients and healthy individuals. The impact of diet on the gut microbiome of prediabetic patients was also assessed in an effort to identify nutrition-based interventions that could potentially prevent the progression of prediabetes to diabetes.
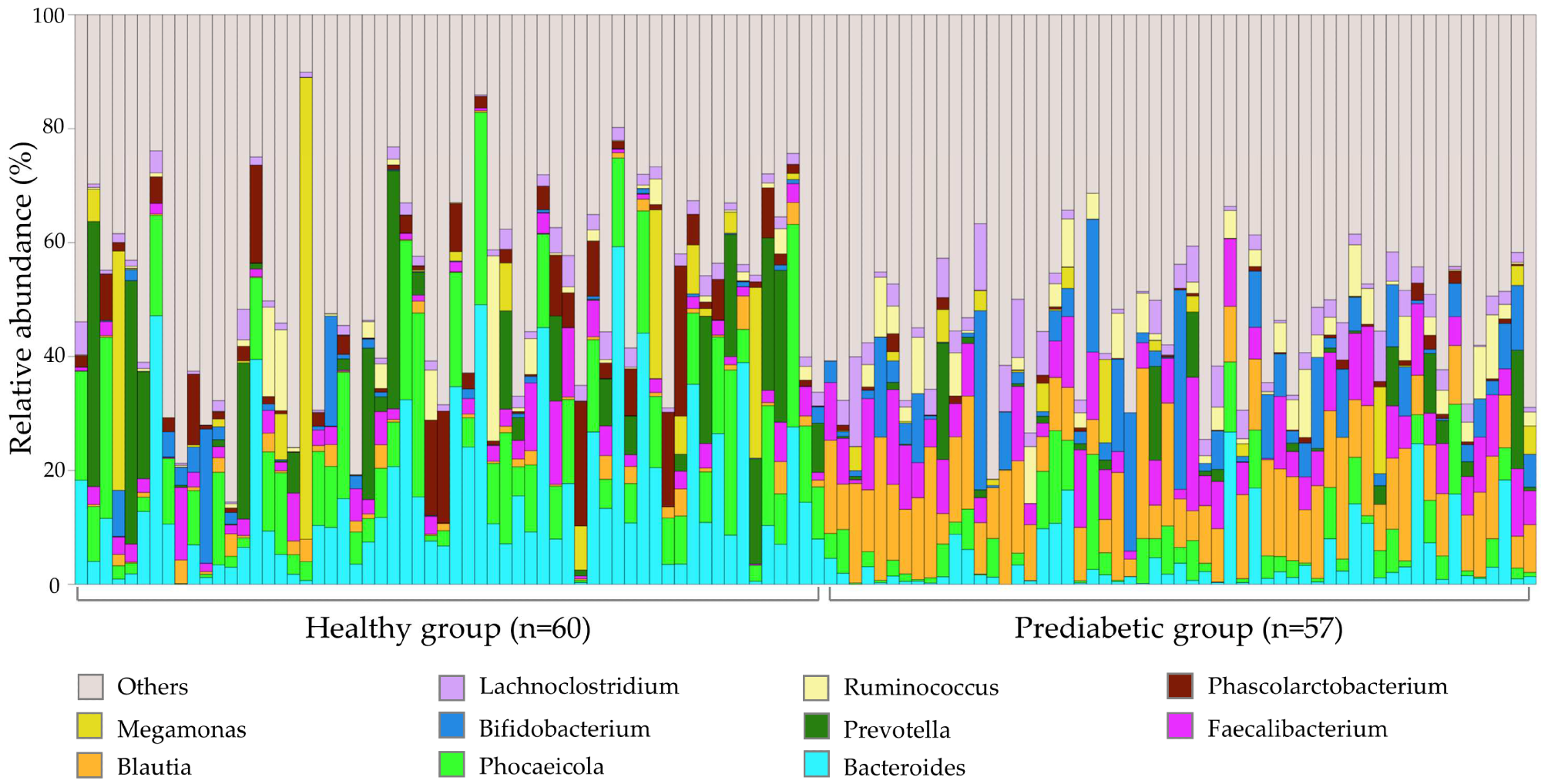
A total of 57 study participants were recruited from Taipei Tzu-Chi Hospital in Taiwan. Gut microbiota data of 60 healthy individuals between 18 and 65 years were obtained from biobanks and used as the reference group.
Study participants were advised to keep a three-day food record and collect fecal samples on the third day. The nutrient composition of the participants’ diet was measured using Nutritionist Professional software 2.0.
Study findings
The composition, diversity, and abundance of the gut microbiota were significantly reduced in prediabetic patients compared to healthy individuals. This finding was in line with previous studies that indicated differential microbial composition in patients with diabetes. Prediabetic patients also exhibited a higher body mass index (BMI) than controls.
Gut microbiome profile of 117 fecal samples at the genus level. The remaining bacterial genera are summed as ‘Others’.
Consistent with previous studies on type 2 diabetes, the current study reported higher levels of Mediterraneibacter, Bifidobacterium, Blautia, Anaerostipes, Clostridium, and Butyricicoccus in the fecal samples of healthy individuals than prediabetic patients.
Previous studies have shown that butyrate maintains the integrity of the intestinal mucosa. This metabolite is synthesized by gut bacteria, namely, Anaerostipes and Faecalibacterium.
Maintaining the integrity of intestinal mucosa can prevent the invasion of pathogenic bacteria in the blood and the destruction of pancreatic β-cells. This finding indicates the indirect role of Anaerostipes and Faecalibacterium in regulating blood glucose levels.
In contrast to prediabetic samples, healthy fecal samples exhibited high levels of Eggerthella and Streptococcus. However, a higher abundance of Phascolarctobacterium, Bacteroides, Paraprevotella, and Parabacteroides was observed in prediabetic fecal samples.
Prediabetic patients exhibited multiple altered physiological metabolic pathways, which affect insulin transmembrane signaling and overexpression of retinoic acid-inducible gene I (RIG-I). This metabolic dysfunction triggers immune cells to attack β cells, affecting blood glucose levels. Previous studies have also indicated that abnormal sphingolipid metabolism leads to insulin resistance and neuronal apoptosis.
Diet plays a vital role in maintaining gut bacterial diversity and abundance. Therefore, prediabetic patients are advised to consume a low carbohydrate (LC) diet with a higher dietary fiber intake. This combination could improve intestinal barrier integrity, thereby preventing the progression of prediabetes to diabetes.
Conclusions
Differential gut microbial composition and abundance were observed in prediabetic patients compared to healthy controls. This difference is also associated with altered metabolic and physiological responses. These findings suggest that improving the gut microbiome could prevent the onset of diabetes by maintaining normal physiological metabolism.
Journal reference:
Chang, W., Chen, Y., Tseng, H., et al. (2024). Gut Microbiota in Patients with Prediabetes. Nutrients16(8); 1105. doi:10.3390/nu16081105
A scanning electron micrograph of Enterococcus faecalis bacteria, which can infect surgical wounds
Science Photo Library/Alamy
Surgical infections could primarily be caused by bacteria that already live on your skin, rather than via external contamination, according to a study of just over 200 people who underwent spinal procedures.
Instead of coming from the hospital environment, many post-surgery infections could stem from an individual’s skin microbiome, says Dustin Long at the University of Washington in Seattle.
To investigate that idea, Long and his colleagues collected skin swabs before and after 204 people underwent different types of spinal surgery.
Fourteen of the participants went on to develop wound infections. After analysing the microbes responsible, the team found that 12 of the cases involved bacteria that were already part of the individuals’ skin microbiomes before surgery.
“Virtually all of the SSIs [surgical site infections] we encountered originated from the patient’s own microbiome, rather than pathogens that were introduced from the hospital or the operating room,” says team member Stephen Salipante, also at the University of Washington.
The researchers expect similar results for any surgery that involves cutting the skin, says Long.
They also found that 59 per cent of the infection-causing organisms uncovered in the study were resistant to pre-surgery antibiotics given intravenously to all the participants, in an effort to prevent such infections. “By characterising the antibiotic resistance traits in the microbiome before surgery, antibiotic therapy could be tailored to each individual patient in order to make it as effective as possible,” says Salipante.
Future research could also look into the most effective methods for sterilising people’s skin before an operation, he says.
Despite the findings, a clean hospital environment and sterile surgical instruments are still essential, says Long.
“Much of the information on the importance of bacterial skin flora in surgical site infection, and particularly surgery involving implantable material, has been known for several decades,” says Roger Bayston at the University of Nottingham in the UK.
Covering the American health care system means we tell some scary stories. This episode of “An Arm and a Leg” sounds like a real horror movie.
It uses one of Hollywood’s favorite tropes: machines taking over. And the machines belong to the private health insurance company UnitedHealth Group.
Host Dan Weissmann talks to Stat News reporter Bob Herman about his investigation into Medicare Advantage plans that use an algorithm to make decisions about patient care. The algorithm is owned by a subsidiary of UnitedHealth Group.
Herman tells Weissmann that some of UnitedHealth’s own employees say the algorithm creates a “moral crisis” in which care is unfairly denied.
Scary stuff! Such reporting even has caught the eye of powerful people in government, putting Medicare Advantage plans under scrutiny.
Previously, Dan was a staff reporter for Marketplace and Chicago’s WBEZ. His work also appears on All Things Considered, Marketplace, the BBC, 99 Percent Invisible, and Reveal, from the Center for Investigative Reporting.
Note: “An Arm and a Leg” uses speech-recognition software to generate transcripts, which may contain errors. Please use the transcript as a tool but check the corresponding audio before quoting the podcast.
Dan: Hey there–
So this is kind of a horror story. But it’s not quite the kind of story it might sound like at first.
Because at first, it might sound like a horror story about machines taking over, making all the decisions– and making terrible, horrifying choices. Very age-of-Artificial Intelligence.
But this is really a story about decisions made by people. For money.
It’s also kind of a twofer sequel– like those movies that pit two characters from earlier stories against each other. Like Godzilla vs King Kong, or Alien vs Predator.
Although in this case, I’ve gotta admit, the two monsters are not necessarily fighting each other.
Let’s get reacquainted with them.
On one side, coming back from our very last episode, we’ve got Medicare Advantage: This is the version of Medicare that’s run by private insurance companies.
It’s got a bright and appealing side, compared to the traditional Medicare program run by the federal government, because: It can cost a lot less, month to month — saving people money on premiums. And it often comes with extra benefits, like dental coverage, which traditional Medicare doesn’t offer. [I know.]
But Medicare Advantage can have a dark side, which is basically: Well, you end up dealing with private insurance companies for the rest of your life. You need something — a test, a procedure, whatever — they might decide not to cover it.
Which can be scary.
Our other returning monster — am I really calling them a monster? — well, last time we talked about them, in 2023, we had an expert calling them a behemoth. That’s United HealthGroup. You might remember, they’re not only one of the biggest insurance companies
— and maybe not-coincidentally the very biggest provider of Medicare Advantage plans —
they’ve also got a whole other business– under the umbrella name Optum. And Optum has spent the last bunch of years buying up a gazillion other health care companies of every kind.
That includes medical practices — they employ more doctors than anyone else, by a huge margin. It includes surgery centers, and home-health companies, and every kind of middleman company you can imagine that works behind the scenes — and have their hands in a huge percentage of doctor bills and pharmacy visits.
A few years ago, United bought a company called NaviHealth, which provides services to insurance companies that run Medicare Advantage plans.
NaviHealth’s job is to decide how long someone needs to stay in a nursing home, like if you’re discharged from a hospital after surgery, but you’re not ready to go home yet.
And the horror story– the stories, as dug up by reporters — starts after United bought NaviHealth.
And according to their reports, it involves people getting kicked out of those nursing homes who aren’t ready to go home.
People getting sent home who can’t walk up the stairs in their house. Who can’t walk at all. Who are on feeding tubes. People who NaviHealth’s own employees are saying, “Wait. This person isn’t ready to go home.”
But their new bosses have told them: You’re not really making these decisions anymore.
This is where machines do enter the picture.
NaviHealth’s distinctive offering has always been its proprietary algorithm– an algorithm that makes predictions about how long any given patient might need to stay.
Before United bought the company, that algorithm was used as a guide, a first-guess. Humans weighed in with their own judgment about what patients needed.
After United bought the company, people inside have told reporters, that changed: The new owners basically told their employees, If the algorithm says someone can go home after x days, that’s when we’re cutting them off.
Like pretty much any horror movie, this story’s got people running around trying to tell everyone: HEY, WATCH OUT! THERE’S SOMETHING BIG AND DANGEROUS HAPPENING HERE.
And in this case, they’ve actually gotten the attention of some people who might have the power to do something about it. Now, what those people will do? We don’t know yet.
And, by the way: Yes, I said at the end of our last episode that we’d be talking about Medicaid this time around. That’s coming! But for now, strap in for this one.
This is An Arm and a Leg, a show about why health care costs so freaking much, and what we can maybe do about it. I’m Dan Weissmann. I’m a reporter, and I like a challenge. So our job on this show is to take one of the most enraging, terrifying, depressing parts of American life, and bring you something entertaining, empowering, and useful.
So. I said that, like every horror movie, this one has people who are seeing what’s going on and are trying to warn everybody?
Like those movies, we’re gonna follow one of those people, watch them discover the problem, see how deep it goes, and start ringing alarm bells. Let’s meet our guy.
Bob Herman: My name is Bob Herman. I’m a reporter at STAT News
Dan: Stat is an amazing medical news publication. Bob covers the business of medicine there. Bob started working on this story in November 2022, after talking to a source who runs nursing homes. Bob’s source was complaining about Medicare Advantage.
Bob Herman: There were a lot of payment denials. They just weren’t able to get paid. And just offhandedly, the source mentioned like, um, you know, and they’re attributing everything to this algorithm. This algorithm said, You know, only 17 days for our patients and then time’s up and I went running to Casey Ross
Dan: Casey is a reporter at Stat who focuses on tech and AI in healthcare. Bob said, hey, what do you think of this? Wanna team up?
Bob Herman: And he was hooked.
Dan: They started talking to people who worked at nursing homes, talking to experts, and talking to families. And it was clear: They were onto something.
Bob Herman: It took so many families by surprise to be like, what do you mean we’re going home? The, you know, my husband, my wife, my grandma, my grandpa, they can’t go to the bathroom on their own. Like, what do you? It was just, it was so confusing to people. It seemed like such a, a cold calculation,
Dan: One person they ended up talking with was Gloria Bent. Her husband Gary was sent to a nursing home for rehab after brain surgery for cancer. He was weak. He couldn’t walk. And he had something called “left neglect”: His brain didn’t register that there was a left side of his body. Here’s Gloria testifying before a Senate committee about how — when Gary arrived at the nursing home — the first thing he got was a discharge date. That is…
Gloria Bent: Before the staff of the facility could even evaluate my husband or develop a plan of care, I was contacted by someone who identified themselves as my Navi Health Care Coordinator
Dan: Gloria says when she told the nursing home staff she’d heard from NaviHealth, they groaned. And told her what to expect.
Gloria Bent: I was told that I had just entered a battlefield, that I could expect a series of notices of denial of Medicare payment accompanied by a discharge date that would be two days after I got that notice.
Dan: Yeah, they said she’d get two days notice. Gloria says the nursing home staff told her she’d have 24 hours to appeal each of those, but even if she won, the denials would keep coming. In fact, they said,
Gloria Bent: If we won a couple of appeals, then we could expect that the frequency with which these denials were going to come would increase.
Dan: All of which happened. NaviHealth started issuing denials July 15, 2022, after Gary had been at the home for a month.
Gloria appealed. She told senators what the doctor who evaluated the appeal found: Gary couldn’t walk. He couldn’t even move — like from bed to a chair — without help from two people.. That reviewer took Gloria’s side.
Her husband’s next denial came a week after the first. Gloria won that appeal too. She says the reviewer noted that Gary needed maximum assistance with activities of daily living.
The third denial came four days later, and this time Gloria lost.
Gary came home in an ambulance: As Gloria testified, he couldn’t get into or out of a car without assistance from someone with special training.
And when he got into the ambulance, he had a fever. The next morning, he wound up in another ambulance — headed to a hospital with meningitis. He lost a lot of the functioning he’d picked up at the nursing home.
He died at home a few months later. When Gloria testified in the Senate, all of it was still fresh. She told them that as awful as Gary’s illness and decline had been, the fights with insurance were an added trauma.
Gloria Bent: This should not be happening to families and patients. It’s cruel. Our family continues to struggle with the question that I hear you asking today. Why are people who are looking at patients only on paper or through the lens of an algorithm
making decisions that deny the services judged necessary by health care providers who know their patients.
Dan: Bob Herman calls Gloria’s story heartbreaking, like so many others he’s seen.
And his attention goes to one part of Gloria’s story beyond denial-by-algorithm.
Because: It’s not just one denial. It’s that series of denials. You can appeal, but as Gloria testified, the denials speed up. And you have to win every single time. The company only has to win once.
I mean, unless you’re ready to get a lawyer and take your chances in court– which, in addition to being a major undertaking, also means racking up nursing home bills and legal bills you may never get reimbursed for, while the court process plays out.
Bob Herman: This appeal system is designed in such a way that people will give up. If you have a job, you know, even if you don’t, and you’re, and you’re also trying to take care of a family member, um, it’s a rigorous monotonous process that will chew people up and spit them out and then the people are inevitably going to give up. And I think in some ways insurers know that.
Dan: Going out on a limb to say: I think so too. So Bob and Casey’s first story on NaviHealth came out in March of 2023. They were the characters in the movie who go, “HEY, I THINK THERE’S SOMETHING REALLY BAD HAPPENING HERE.”
And people started paying attention. Like the U.S. Senate. which held that hearing where Gloria Bent told her story.
And like the federal agency that runs Medicare — the Centers for Medicare and Medicaid Services, CMS.
CMS finalized a rule that told insurers: You can’t deny care to people just from using an algorithm.
And something else happened too: Bob and Casey started suddenly getting a lot MORE information.
Bob Herman: We received so many responses from people and it just opened the floodgates for former employees, just patients and family members, just everyone across the board.
Dan: And not just former employees. Current employees. And what they learned was: There was absolutely a strategy at work in how this algorithm was being used. It was strategy some people on the inside didn’t feel good about.
And this strategy got developed after United HealthGroup — and its subsidiary, Optum– bought NaviHealth in 2020. And here’s what NaviHealth employees started telling Casey and Bob about that strategy.
Bob Herman: For some of us, it’s creating this moral crisis. Like we know that we are having to listen to an algorithm to essentially kick someone out of a nursing home, even though we know that they can barely walk 20 feet.
Dan: What Bob and Casey learned from insiders– and how it connects to United’s role as a health care behemoth– that’s next.
This episode of An Arm and a Leg is produced in partnership with KFF Health News. That’s a nonprofit newsroom covering healthcare in America. Their reporters do amazing work, and I’m honored to work with them. We’ll have a little more about KFF Health News at the end of this episode.
So, NaviHealth — the company with the algorithm — got started in 2015.. And the idea behind it was to use data to get people home faster from nursing homes if they didn’t actually need to be there.
Because there was a lot of evidence that some people were being kept longer than they needed.
Bob Herman: There is some validity to the idea that there’s, there’s wasteful care in Medicare, like, you know, there’s been cases in the past proving that people stay in a nursing home for way longer than is necessary. And obviously there’s financial incentives for nursing homes to keep people as long as possible.
Dan: Traditional Medicare does have limits on nursing home care — but if you need “post-acute care” — help getting back on your feet after leaving a hospital traditional Medicare pays in full for 20 days– pretty much no questions asked. One of the selling points of Medicare Advantage — like selling points to policy nerds and politicians — was that it could cut waste, by asking those kinds of questions. NaviHealth and its algorithm were designed to help Medicare Advantage plans ask those questions in a smart way.
Bob Herman: There were… a lot of believers within NaviHealth that were like, okay, I think we’re doing the right thing. We’re trying to make sure people get home sooner because who doesn’t want to be at home.
Dan: And as those employees told Bob and Casey: Before United and Optum came in, the algorithm had been there as a guide — a kind of first guess — but not the final word.
NaviHealth has staff people who interact directly with patients. And back in the day, the pre-United day, Bob and Casey learned that those staff could make their own judgments.
Which made sense, because the algorithm doesn’t know everything about any individual case. It’s just making predictions based on the data it has.
Bob Herman: And there was just, just this noticeable change after United and OptiMentor that it felt more rigid. There’s no more variation.
Dan: If the algorithm says you go, you are pretty much going.
Bob Herman: United has said, no, that’s not the case, but obviously these documents and other communications that we’ve gotten kind of say otherwise.
Dan: Because these employees weren’t just talking. They were sharing. Internal memos. Emails. Training materials. All making clear: The company wanted people shipped out on the algorithm’s timetable.
Bob Herman: Documents came in showing that like this was a pretty explicit strategy. You know, UnitedHealth was telling its employees. Listen, we have this algorithm. We think it’s really good. So when it tells you how many, how many days someone should be in a nursing home, stick to it.
Dan: Stick to it or maybe be fired. Bob and Casey got documents — employee performance goals– saying: How close you stick to the algorithm’s recommendations? That’s part of how we’re evaluating your job performance.
Bob Herman: It’s okay. Algorithm said 17 days, you better not really go outside of that because your job is on the line.
Dan: Here’s how closely people were expected to stick to it. In 2022, employee performance goals shared with STAT showed that workers were expected to keep actual time in nursing homes to within three percent of what the algorithm said it should be. Across the board.
So, say you had 10 patients, and the algorithm said they each should get 10 days. That’s 100 days. Your job was to make sure that the total actual days for those patients didn’t go past 103 days.
Then, in 2023, the expectations got more stringent: Stay within one percent of the algorithm’s predictions. 10 patients, the algorithm says 100 days total? Don’t let it get past a hundred and one.
Bob Herman: Like that is, almost nothing. Like what, what, your hands are tied. If you’re that employee, what are you going to do? Are you going to get fired? Are you going to do what you’re told?
Dan: And one person who ended up talking, to did get fired.
Bob Herman: Correct. Yes. Uh, Amber Lynch did get fired And what she said was what we had also heard just more broadly was it, it created this internal conflict, like, Oh my God, what I’m doing doesn’t feel right.
Dan: Amber Lynch was a case manager. She told Bob and Casey about onepatient who couldn’t climb the stairs in his home after knee surgery. But the algorithm said he was ready. Amber’s supervisor said, “Have you asked the nursing home staff if they’ve tried to teach him butt bumping?” Amber grit her teeth and made the suggestion to the rehab director.
Amber Lynch: And she looked at me like I had two heads. She’s like, he is 78 years old. He’s not going to do that. He’s not safe to climb the stairs yet. He’s not doing it. We’re not going to have it butt bump the stairs.
Dan: Amber told Bob and Casey that when she got fired, it was partly for failing to hit the one percent target and partly for being late with paperwork– which she told Bob and Casey she fell behind because her caseload was so heavy.
She wasn’t the only one with that complaint.
Bob and Casey’s story shows another NaviHealth case manager– not named in the story because they’re still on the job — in their home office, struggling to keep up.
That week, they were supposed to work with 27 patients and their families. Gather documents, hold meetings. Another week, shortly before, they’d had 40 patients.
“Do you think I was able to process everything correctly and call everyone correctly the way I was supposed to?” the case manager asked. “No. It’s impossible. No one can be that fast and that effective and capture all of the information that’s needed.”
Bob and Casey watched this case manager fill out a digital form, feeding the algorithm the information it asked for on a man in his 80s with heart failure, kidney disease, diabetes and trouble swallowing, who was recovering from a broken shoulder.
A few minutes later, the computer spat out a number: 17 days.
The case manager didn’t have a lot of time or leeway to argue, but they were skeptical that the algorithm could get that number exactly right based on only the data it had.
And what data is the algorithm working with? What’s it comparing the data on any given patient TO? Bob Herman says that’s a big question.
Bob Herman: It’s something that for sure, like Casey and I, it’s been bothering us. Like, what, how is this whole system? Like, what is it based on? And we were never really given straight answers on that. NaviHealth and Optum and United have said it’s based on millions of patient records over time. The sources of that, it’s, it’s a little unclear, where all that’s coming from.
Dan: Bob and Casey talked with an expert named Ziad Obermeyer, a professor at the University of California Berkeley School of Public Health, who is not anti-algorithm. He actually builds algorithmic tools for decision making in public health.
AND he’s done research showing that some widely-used algorithms just scale up and automate things like racial bias.
He told Bob and Casey: Using an algorithm based on how long other, earlier patients have stayed in a nursing home — that’s not a great idea.
Because people get forced out of nursing homes, in his words, “because they can’t pay or because their insurance sucks.” He said, “So the algorightm is basically learning all the inequalities of our current system.”
And leaving aside that kind of bias, it seems unlikely to Bob that any algorithm could predict exactly what every single patient will need every single time.
No matter how much data it’s got, it’s predicting from averages.
Bob Herman: It reminds me of, like, a basketball game where let’s say someone averages 27 points per game. They don’t have 27 points every single, the game they go out there. It just varies from time to time.
Dan: But the NaviHealth algorithm doesn’t have to be right every time for United to make money using it.
Using it to make decisions can allow United to boost profits coming and going.
Bob Herman: United health and the other insurance companies that use Navi health. Are using this technology to more or less kick people out of nursing homes before they’re ready. And that is the claims denial side where it’s like, okay, let’s save as much money as we can instead of having to pay it to a nursing home.
Dan: And that’s just one side of it. The insurance side. Claims denial. But United isn’t just in the insurance business.
United’s Optum side is in every other part of health care.
Including — in the years since United took over NaviHealth — home health services. The kind of services you’re likely to need when you leave a nursing home.
In 2022, Optum bought one top home health company in what one trade publication called a “monster, jaw-dropping mega-deal” — more than 5 billion dollars. In 2023, Optum made a deal to buy a second mega-provider.
Bob and Casey’s story says NaviHealth’s shortening nursing home stays is integral to United’s strategy for these acquisitions. It does seem to open up new opportunities.
Bob Herman: You’re out of the nursing home because our algorithm said so. Now we’re going to send you to a home health agency or we’re going to send some home health aides into your home. And by the way, we own them.
Dan: Oh, right, because: If you’re in a Medicare Advantage plan, your insurer can tell you which providers are covered.
Bob Herman: So the real question becomes, how much is United potentially paying itself?
Dan: That is: How much might United end up taking money out of one pocket — the health insurance side — and paying itself into another pocket, Optum’s home-health services?
We don’t know the answer to how much United is paying itself in this way, or hoping to. And United has said its insurance arm doesn’t favor its in-house businesses.
But it seems like a reasonable question to ask. Actually, it’s a question the feds seem to be asking.
Optum hasn’t wrapped up its purchase of that second home-health company yet, and in February 2024, the Wall Street Journal and other outlets reported that the U.S. Department of Justice had opened an anti-trust investigation.
And you don’t have to be in a Medicare Advantage plan run by United to get kicked out of a nursing home on an algorithm’s say-so.
Bob Herman says NaviHealth sells its algorithm-driven services to other big insurance companies
He says, put together, the companies that use NaviHealth cover as many as 15 million people — about half of everybody in Medicare Advantage.
Bob Herman: Odds are, if you’re in a Medicare Advantage plan, there’s a, there’s a really good shot that your coverage policies, if you get really sick and need nursing home care, for example, or any kind of post acute care, an algorithm could be at play at some point.
Dan: This is the dark side of Medicare Advantage.
Bob Herman: Everyone loves their Medicare Advantage plan when they first sign up, right? Because it’s offering all these bells and whistles. It’s, here’s a gym membership. It’s got dental and vision, which regular Medicare doesn’t have. And it’s also just, it’s, it’s cheaper. Like, if it’s just from a financial point of view, if, if you’re a low income senior, How do you turn it down? There’s, there’s so many plans that offer like free, there’s no monthly premiums in addition to all the bells and whistles. But Nobody understands the trade offs , When you’re signing up for Medicare and Medicare Advantage, you’re on the healthier side of, of being a senior, right?
Dan: And none of us can count on staying healthy forever. When you sign up for Medicare you’re signing up your future self — whether that’s ten or twenty or more years out. That future you, might really need good medical care.
And at that point, as we explained in our last episode, if Medicare Advantage isn’t working for you, you may not be able to get out of it.
Bob Herman: You could potentially not fully get the care that you need. We shouldn’t assume that, that this couldn’t happen to us because it can.
Dan: So, yeah. Kind of a horror story. But: Unlike some horror movies, when Bob and Casey started publishing their stories, they started getting people’s attention.
We mentioned the new rules from the feds and the senate hearings after Bob and Casey’s first story in March 2023
Later in the year, when Bob and Casey published their story with documents and stories from inside NaviHealth, a class-action lawsuit got filed.
Since then, CMS has said it will step up audits under its new rules.
Bob Herman: There was a memo that CMS sent out to Medicare advantage plans that said, Hey, listen, we’re telling you again, do not deny care solely on any AI or algorithms. Like just don’t do it.
Dan: And in February 2024, the Senate held another hearing.
Here’s Senator Elizabeth Warren at that hearing, saying these CMS rules aren’t enough. We need stronger guardrails.
Elizabeth Warren: Until CMS can verify that AI algorithms reliably adhere to Medicare coverage standards by law, then my view on this is CMS should prohibit insurance companies from using them in their MA plans for coverage decisions. They’ve got to prove they work before they put them in place.
Dan: So people — people with at least some power– are paying some attention.
Bob Herman: I don’t think this is necessarily going to escape. Political scrutiny for a while.
Dan: So, basically, the story isn’t over.
This isn’t one of those horror movies where the monster’s been safely defeated at the end, and everybody just starts cleaning up the mess. And it’s not one where the monster is just on the loose, unleashing the apocalypse.
Because it’s not a movie. There’s no ending. There’s just all of us trying to figure out what’s going on, and what we can maybe do about it.
One last thing: I got a lot of emails after our last episode, where we laid out a lot of information about Medicare Advantage and traditional Medicare. Most of it was along the lines of, Thank you! That was really helpful! Which made me feel really good.
And we got a couple notes about things we could have done better. Especially this: We said Traditional Medicare leaves you on the hook for 20 percent of everything, without an out of pocket limit.
Which is true — but only for Medicare Part B: Doctor visits, outpatient surgeries and tests. Which can add up, for sure.
Medicare Part A — if you’re actually hospitalized — covers most services at 100 percent, after you meet the deductible. In 2024 that’s one thousand, six hundred thirty-two dollars.
Thanks to Clarke Lancina for pointing that out.
There have been a bunch of other, amazing notes in my inbox recently, and I want to say: Please keep them coming.
If you go to arm and a leg show dot com, slash, contact, whatever you type there goes straight to my inbox. You can attach stuff too: documents… voice memos.
Please let me hear from you. That’s arm and a leg show dot com, slash contact.
I’ll catch you in a few weeks.
Till then, take care of yourself.
This episode of an arm and a leg was produced by me, Dan Weissmann, with help from Emily Pisacreta, and edited by Ellen Weiss.
Adam Raymonda is our audio wizard. Our music is by Dave Weiner and blue dot sessions. Extra music in this episode from Epidemic Sound.
Gabrielle Healy is our managing editor for audience. She edits the first aid kit newsletter.
Bea Bosco is our consulting director of operations. Sarah Ballama is our operations manager.
And Arm and a Leg is produced in partnership with KFF Health News. That’s a national newsroom producing in depth journalism about healthcare in America and a core program at KFF, an independent source of health policy research, polling and journalism.
Zach Dyer is senior audio producer at KFF Health News. He’s editorial liaison to this show.
And thanks to the Institute for Nonprofit News for serving as our fiscal sponsor, allowing us to accept tax exempt donations. You can learn more about INN at INN. org.
Finally, thanks to everybody who supports this show financially– you can join in any time at arm and a leg show dot com, slash, support — and thanks for listening.
“An Arm and a Leg” is a co-production of KFF Health News and Public Road Productions.
To keep in touch with “An Arm and a Leg,” subscribe to the newsletter. You can also follow the show on Facebook and the social platform X. And if you’ve got stories to tell about the health care system, the producers would love to hear from you.
To hear all KFF Health News podcasts, click here.
And subscribe to “An Arm and a Leg” on Spotify, Apple Podcasts, Pocket Casts, or wherever you listen to podcasts.
Combining pelvic floor exercises with behavioral therapy could be more effective than current medical treatments at helping men with frequent urges to urinate, new research in men has found.
The initial results from the Bladder Emptying Disorder Therapy (BEST) Trial are presented today [Monday 8 April 2024] at the European Association of Urology Congress in Paris. They reveal that an app-based therapy leads to significant improvements in the lower urinary tract symptoms that many millions of men experience – hesitancy, straining, frequent urges to urinate and emptying the bladder effectively. Full results of the trial are expected to be published later this year.
Carried out in Germany, this is the world’s first randomised controlled trial to look at combining pelvic floor training, behavioural therapy and bladder control techniques for mild, moderate and severe bladder emptying disorders in men, all delivered as an app-based therapeutic.
Bladder emptying disorders can start to appear from the age of 30 and typically affect a large proportion of men aged over 50.
While clinical guidelines recommend physiotherapy, behavioural therapy and lifestyle changes as a first-line of treatment, they are often neglected by clinicians due to a lack of available evidence. Several unpleasant side effects are associated with the few drugs available, and surgery is only advised for those with severe symptoms.
Professor Christian Gratzke, from University Hospital Freiburg in Germany, who co-led the trial, explains: “Frequent urges to urinate and issues emptying the bladder are the most prevalent urinary conditions we see in men after urinary tract infections. While some drugs are available, they don’t tend to be effective, and up until now there’s been little data available to back physiotherapy. We’re confident that we now have that data, and making this form of therapy available digitally could be a game changer for the millions of men who struggle day-to-day with issues emptying their bladder.”
The researchers recruited 237 men aged over 18 from across Germany into their 12-week study. Half the men were randomised to receive standard medical care, while the other half were given access to the Kranus Lutera app-based therapy alongside standard care. These participants were asked to record a urination diary, which was used to inform their treatment, and complete questionnaires about the severity of their symptoms and their overall quality of life.
After 12 weeks, the trial found significant and clinically meaningful improvements in symptoms and quality of life measures from participants given the app-based therapy, who reported an average seven-point increase in symptom scores compared to those in the control group.
Crucially, the study found that the app-based therapy was more effective than medical therapy. No patients reported any side-effects or challenges accessing the smartphone app.
The findings challenge the dogma of the 1980’s and 1990’s, when prostrate surgery was the first line of treatment for an overactive bladder, and offer a welcome alternative to drugs, say the researchers.
“Many men with bladder emptying disorders are ageing and have other medical conditions that require drug treatments,” says Professor Gratzke. “The limited drugs we have available aren’t suitable for these patients due to their side effects. For those with mild-to-moderate urinary symptoms, this digital therapy is without side effects and improves symptoms by a magnitude we have not seen before. Simply strengthening the pelvic floor makes all the difference, it’s a no brainer.”
There has been little to no evidence to support training men to better control their bladders, despite this being recommended in clinical guidelines. This is the first randomised controlled trial looking at physiotherapy and behavioural therapy for bladder emptying disorders, and it shows a very positive effect over conventional drug treatment.
We now need a bigger trial looking at the longer-term effect of this app-based therapy after 12 weeks for different forms of bladder emptying disorders. If offered widely, this treatment could dramatically change clinical practice, and could relieve symptoms without exposing patients to drugs. We could save a lot of unnecessary prescriptions for drugs that tend to be of little benefit.”
Jean-Nicolas Cornu, Professor of Urology at the Charles Nicolle Hospital in France and member of the EAU Scientific Congress Office
The researchers compared data from men whose symptoms were due to overactive bladder with those whose symptoms were due to an enlarged prostate. They found that both groups benefited from the therapy. However, it did not compare the effect of therapy on different forms of bladder emptying disorder.
The research was funded by Kranus Health who was independent of the trial.
When the FDA recently convened a committee of advisers to assess a cardiac device made by Abbott, the agency didn’t disclose that most of them had received payments from the company or conducted research it had funded — information readily available in a federal database.
One member of the FDA advisory committee was linked to hundreds of payments from Abbott totaling almost $200,000, according to a database maintained by the Department of Health and Human Services. Another was connected to 100 payments totaling about $100,000 and conducted research supported by about $50,000 from Abbott. A third member of the committee worked on research supported by more than $180,000 from the company.
The government database, called “Open Payments,” records financial relationships between doctors and certain other health care providers and the makers of drugs and medical devices. KFF Health News found records of Abbott payments associated with 10 of the 14 voting members of the FDA advisory panel, which was weighing clinical evidence for a heart device called TriClip G4 System. The money, paid from 2016 through 2022 — the most recent year for which the database shows payments — adds up to about $650,000.
The panel voted almost unanimously that the benefits of the device outweigh its risks. Abbott announced on April 2 that the FDA had approved TriClip, which is designed to treat leakage from the heart’s tricuspid valve.
The Abbott payments illustrate the reach of medical industry money and the limits of transparency at the FDA. They also shed light on how the agency weighs relationships between people who serve on its advisory panels and the makers of drugs and medical devices that those committees review as part of the regulatory approval process.
The payments do not reflect wrongdoing on the part of the agency, its outside experts, or the device manufacturer. The database does not show that any of the payments were related directly to the TriClip device.
But some familiar with the process, including people who have served on FDA advisory committees, said the payments should have been disclosed at the Feb. 13 meeting — if not as a regulatory requirement, then in the interest of transparency, because the money might call into question committee members’ objectivity.
“This is a problem,” Joel Perlmutter, a former FDA advisory committee member and a professor of neurology at Washington University School of Medicine in St. Louis, said by email. “They should or must disclose this due to bias.”
The Open Payments database records several kinds of payments from drug and device makers. One category, called “associated research funding,” supports research in which a physician is named a principal investigator in the database. Another category, called “general payments,” includes consulting fees, travel expenses and meals connected to physicians in the database. The money can flow from manufacturers to third parties, such as hospitals, universities, or other corporate entities, but the database explicitly connects doctors by name to the payments.
At the public meeting to consider the TriClip device, an FDA official announced that committee members had been screened for potential financial conflicts of interest and found in compliance with government requirements.
FDA spokesperson Audra Harrison said by email that the agency doesn’t comment on matters related to individual advisory committee members.
“The FDA followed all appropriate procedures and regulations in vetting these panel members and stands firmly by the integrity of the disclosure and vetting processes in place,” she said. “This includes ensuring advisory committee members do not have, or have the appearance of, a conflict of interest.”
Abbott “has no influence over who is selected to participate in FDA advisory committees,” a spokesperson for the company, Brent Tippen, said in a statement.
Diana Zuckerman, president of the National Center for Health Research, a think tank, said the FDA shouldn’t have allowed recipients of funding from Abbott in recent years to sit in judgment of the Abbott product. The agency takes too narrow a view of what should be disqualifying, she said.
One committee member was Craig Selzman, chief of the Division of Cardiothoracic Surgery at the University of Utah. The Open Payments database connects to Selzman about $181,000 in associated research funding from Abbott to the University of Utah Hospitals & Clinics.
Asked in an interview if a reasonable person could question the impartiality of committee members based on the Abbott payments, Selzman said: “People from the outside looking in would probably say yes.”
He noted that Abbott’s money went to the university, not to him personally. Participating in industry-funded clinical trials benefits doctors professionally, he said. He added: “There’s probably a better way to provide transparency.”
The FDA has a history of appointing people to advisory committees who had relationships with manufacturers of the products under review. For example, in 2020, the doctor who chaired an FDA advisory committee reviewing Pfizer’s covid-19 vaccine had been a Pfizer consultant.
Appearance issues
FDA advisory committee candidates, selected to provide expert advice on often complicated drug and device applications, must complete a confidential disclosure report that asks about current and past financial interests as well as “anything that would give an ‘appearance’ of a conflict.”
The FDA has discretion to decide whether someone with an “appearance issue” can serve on a panel, according to a guidance document posted on the agency’s website. Relationships more than a year in the past generally don’t give rise to appearance problems, according to the document, unless they suggest close ties to a company or involvement with the product under review. The main question is whether financial interests would cause a reasonable person to question the member’s impartiality, the document says.
The FDA draws a distinction between appearance issues and financial conflicts of interest. Conflicts of interest occur when someone chosen to serve on an advisory committee has financial interests that “may be impacted” by their work on the committee, an FDA explainer says.
If the FDA finds a conflict of interest but still wants the applicant on a panel, it can issue a public waiver. None of the panelists voting on TriClip received a waiver.
The FDA’s approach to disclosure contrasts with rules for conferences at which doctors earn credit for continuing medical education. For example, for a recent conference in Boston on technology for treatment of heart failure, including TriClip, the group holding the meeting directed speakers to include in their slide presentations disclosures going back 24 months.
Those disclosures — naming companies from which speakers had received consulting fees, grant support, travel expenses, and the like — also appeared on the conference website.
‘Unbridled enthusiasm‘
The FDA has designated TriClip a “breakthrough” device with “the potential to provide more effective treatment or diagnosis of a life-threatening or irreversibly debilitating disease” compared with current treatments, an agency official, Megan Naber, told the advisory committee.
Naber said that for breakthrough devices, the “totality of data must still provide a reasonable assurance of safety and effectiveness” but the FDA “may be willing to accept greater uncertainty” about the balance of risks and benefits.
In a briefing paper for the advisory committee, FDA staff pointed out findings from a clinical trial that didn’t reflect well on TriClip. For example, patients treated with TriClip had “numerically higher” mortality and heart failure hospitalization rates during the 12 months after the procedure compared with a control group, according to the report. Tippen, the Abbott spokesperson, didn’t respond to a request for comment on those findings.
The committee voted 14-0 that TriClip was safe for its intended use. The panel voted 12-2 that the device was effective, and it voted 13-1 that the benefits of TriClip outweighed the risks.
The committee member to whom the database attributes the most money from Abbott, Paul Hauptman, cast one of the votes against the device on effectiveness and the sole vote against the device on the bottom-line question of its risks versus benefits.
Hauptman said during the meeting that the question of safety was “very, very clear” but added: “I just felt the need to pull back a little bit on unbridled enthusiasm.” Who will benefit from the device, he said, “needs better definition.”
Hauptman, dean of the University of Nevada-Reno School of Medicine, is connected to 268 general payments from Abbott totaling about $197,000 in the Open Payments database. Some payments are listed as going to an entity called Keswick Cardiovascular.
Hauptman said in an email that he followed FDA guidance and added, “My impartiality speaks for itself based on my vote and critical comments.”
Some committee members voted in favor of the device despite concerns.
Marc Katz, chief of the Division of Cardiothoracic Surgery at the Medical University of South Carolina, is linked to 77 general payments totaling about $53,000 from Abbott and worked on research supported by about $10,000 from the company, according to Open Payments.
“I voted yes for safety, no for effectiveness, but then caved and voted yes for the benefits outweighing the risks,” he said in the meeting.
In an email, he said of his Abbott payments: “All was disclosed and reviewed by the FDA.” He said that he “can be impartial” and that he “openly expressed … concerns about the treatment.”
Mitchell Krucoff, a professor at Duke University School of Medicine, is connected to 100 general payments totaling about $105,000. Some went to a third party, HPIC Consulting. He also worked on research supported by about $51,000 from Abbott, according to Open Payments.
He said during the meeting that he voted in favor of the device on all three questions and added that doctors have “a lot to learn” once it’s on the market. For instance: By using the device to treat patients now, “do we set people up for catastrophes later?”
In an email, Krucoff said he completed a “very thorough conflict of interest screening by FDA for this panel,” which focused not only on Abbott but also on “any work done/payments received from any other manufacturer with devices in this space.”
John Hirshfeld Jr., an emeritus professor of medicine at the University of Pennsylvania, is linked by the database to six general payments from Abbott totaling $6,000. Two of the payments linked to him went to a nonprofit, the Cardiovascular Research Foundation, according to the database. He voted yes on all three questions about TriClip but said at the meeting that he “would have liked to have seen more rigorous data to support efficacy.”
In an email, Hirshfeld said he disclosed the payments to the FDA. The agency did not deem him to have a conflict because he had no stake in Abbott’s success and his involvement with the company had ended, he said. Through the conflict-of-interest screening process, he said, he had been excluded from prior advisory panels.
This article was reprinted from khn.org, a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF – the independent source for health policy research, polling, and journalism.