The surgery to implant a genetically modified pig’s liver into the 71-year-old man lasted 8 hours.Credit: David Tadevosian/Shutterstock
A 71-year-old man in China has become the first living person to receive a liver transplant from a genetically modified pig — and the fifth person reported to have received a pig organ. More than two weeks after the surgery, the man is “doing very well”, says Sun Beicheng, a surgeon at the First Affiliated hospital of Anhui Medical University who led the transplantation.
The surgeons have not released many details about the procedure, but researchers are encouraged by the apparent success. “It is very exciting news,” says Burcin Ekser, a transplant surgeon at Indiana University School of Medicine in Indianapolis.
The liver is the latest in a series of pig organs introduced to people. Since early 2022, surgeons have transplanted pig hearts, kidneys and a thyroid into four people. Three died in the months after receiving their transplants, and researchers say their pre-existing poor health, which contributed to their selection as transplant candidates, makes it difficult to determine whether the transplants were a factor. One person who was operated on in mid-April is still alive today.
The transplants have allowed researchers to gain valuable insights into the feasibility of xenotransplantation — the transfer of organs from one species to another. Clinicians hope the technology might one day supply organs for the thousands of people who die waiting for a donor organ each year.
Xenotransplantation of livers has experienced a surge this year. In January 2024, a US team connected a genetically modified pig liver outside the body of a clinically dead person. In March, Kefeng Dou, a transplant surgeon at Xijing Hospital of the Air Force Medical University in Xi’an and his colleagues transplanted a genome-edited pig liver into a clinically dead individual for 10 days, as agreed with the man’s family, and saw no signs of rejection. And earlier in May, another team in China transplanted a pig kidney and liver into a clinically dead person.
Right lobe
In the most recent pig-organ transplant, the recipient had a large tumour on the right lobe of his liver, which had not yet spread to other parts of the body. The individual was not eligible to receive a human liver transplant because tests indicated that his liver was functioning too poorly to ensure a good outcome, and his left lobe alone would not be able to keep him alive, says Sun. The doctors didn’t know “when the tumour would rupture”, he says. The situation was “very dangerous”. With few other options, Sun says the patient and his family expressed interest in the xenotransplant. The surgery team say they obtained approval from their hospital’s ethics and transplantation committees on compassionate grounds.
On May 17, in an operation that lasted eight hours, surgeons removed the individual’s right lobe. They replaced it with a 514-gram liver from an 11-month-old miniature pig, weighing 32 kilograms.
The pig had ten genetic modifications to prevent its organs from being rejected soon after being transplanted, says Hong-Jiang Wei at Yunnan Agricultural University, in Kunming, whose team developed the pig. The team deactivated three genes that contribute to the production of sugars on the surface of pig cells, which the human immune system attacks, and introduced seven genes that express human proteins.
Sun says that in tests of the pig liver, they did not detect the presence of porcine cytomegalovirus, which could have contributed to complications in a recipient of a pig heart, who died two months after the procedure.
Save or support
Once the surgeons had re-established blood flow to the transplanted pig liver, it instantly began to secrete bile. From 10 millilitres on the first day, bile production gradually increased to between 200–300 mL on day 13 (a healthy person secretes at least 400 mL of bile a day). Sun says that he has not seen signs of the organ being rejected, including from a biopsy conducted on day 12. “He has normal liver function,” says Sun.
“That is a very positive result,” says Jay Fishman, a specialist in transplant infectious disease at Massachusetts General Hospital in Boston. “In general you don’t see those kinds of good signs if the organ is suffering rejection.”
Livers tend to experience less rejection and injury than a kidney, heart or lung, says Fishman. Although he cautions that signs of chronic rejection could appear later.
In addition to bile, Sun says the pig liver is producing pig versions of albumin and coagulation factors. From the way these essential proteins function, “we may learn a great deal”, says David Cooper, a xenotransplant immunologist at Massachusetts General Hospital in Boston. If the researchers identify that the pig versions of these proteins do not serve the needs of the recipient, future transplants might genetically manipulate the pigs to produce the human versions.
At day 10, Sun says the team had not yet seen signs of liver growth, but that they remain optimistic. He says they hope that ultimately the person’s left lobe will grow large enough to provide full liver function and that the pig liver will serve as a bridge to get to that point.
Oncologist Todd Fehniger researches natural-killer-cell therapy for use in cancer treatment.Credit: David Russler-Germain
As part of a study published in January, 37 people who had been through various failed treatments for blood cancer received infusions of genetically enhanced immune cells that researchers hoped would clear their disease1. The concept was not new — therapies based on T cells have been approved since 2017. But the source of the cells was.
Researchers at the MD Anderson Cancer Center in Houston, Texas, used frozen donor umbilical-cord blood to grow and prepare a lesser-known component of the immune system: natural killer (NK) cells. In the phase I/II trial, 68% of people with B-cell lymphoma who received the cells survived for at least one year — suggesting that the NK-based therapy could work as well as currently available T-cell therapies2. And NK cells seemed to trigger fewer side effects, which have limited the availability of therapies that use chimeric antigen receptor (CAR) T cells, says Katy Rezvani, an oncologist and immunologist at the MD Anderson Cancer Center who led the recent NK-cell study.
Nature Outlook: Cancer treatment
CAR-T therapy requires the extraction of an individual’s own T cells and a two-to-four week wait for the cells to be engineered. After the cells are injected back into individuals, at least one-third of recipients develop cytokine release syndrome, in which a rush of inflammatory molecules causes fever, low blood pressure and other symptoms requiring hospitalization. About one-quarter also develop neurotoxicity, which can be life-threatening3. All of this makes the price of therapy high — around US$400,000 — and limits it to people who are able to withstand the side effects.
So in 2013, at a time when all eyes were on T cells, Rezvani shifted her research focus to NK cells. NK cells have a better safety record and unique features that make them good candidates for off-the-shelf therapies, in which cells from an unrelated donor are prepared ahead of time and frozen, ready to use in anyone. This would save time and money and be a game changer for people who are too unwell to have their own cells extracted. The advantages of NK cells first piqued cancer researchers’ interest two decades ago, but issues such as the cells’ inability to last long in the body hindered development. In the past few years, strategies to take on this challenge have delivered encouraging results in clinical trials.
There are now at least 50 companies testing a wide variety of tactics to give NK cells an edge as a cancer therapy. Several have started phase I trials to test CAR-NK cells like Rezvani’s, grown from a variety of sources including cord blood, induced pluripotent stem cells and cell lines. Other groups, meanwhile, are developing drugs that restore the cancer-killing abilities of NK cells that are already in the body.
“The number of NK companies has just exploded,” says Todd Fehniger, an oncologist at Washington University School of Medicine in St. Louis, Missouri. As researchers test their ideas in early clinical trials, the field is anxious to see which approach, if any, will give people long-lasting results. “We’re still at this inflection point in the field where we need that one clinical success, that one regulatory approval that will spark this torrent of interest,” Fehniger says.
Perked-up persistence
NK cells are well-positioned to steal the immunotherapy spotlight away from T cells. NK cells are equipped with cancer-detecting receptors (see ‘Killer at work’). They got their name in the 1970s for their ability to spot infected and cancerous cells, release molecules that poke holes in cell membranes and trigger their targets’ own self-destruction. NK cells also have a reputation for keeping cancer at bay: one study linked high NK-cell activity to a lower likelihood of developing cancer over the subsequent decade4.
Source: A. Merino et al. Blood Rev.60, 101073 (2023).
What really drew Rezvani in, however, was the safety of these cells. NK cells can’t kill other cells until they integrate a combination of activating and inhibitory signals from dozens of receptors; this constraint prevents them from harming healthy cells. Once activated, NK cells don’t replicate in huge numbers like T cells do, making them much less likely to kick off cytokine release syndrome or graft-versus-host disease, a sometimes-fatal condition in which donor cells attack a transplant recipient’s tissues.
But many of the features that contribute to the safety of using NK cells have also hindered their success as a cancer treatment. In studies done in the 2000s, NK cells from donors lasted only one or two weeks before participants’ immune systems cleared them out5. “There was scepticism that NK cells were not going to be as effective as T cells and I think those scepticisms were well justified. The big problem was their limited persistence,” Rezvani says.
Researchers can extend that persistence by giving people IL-2, an NK-activating cytokine. But IL-2 can be given only at low doses because it can be toxic. IL-2 also stimulates T regulatory (Treg) cells, which hamper anti-tumour immunity and NK-cell activity. In the past decade, another cytokine, IL-15, has gained attention as a more specific way to activate NK cells. Rezvani’s group found that engineering CAR-NK cells to coexpress IL-15 improved their metabolic fitness, which increased their numbers and longevity inside the body6. In the recent trial1 conducted by Rezvani and her team, the engineered CAR-NK cells could still be found in some participants’ blood a year after the treatment.
The study also revealed important variables about the cell source that affected NK-cell activity. People who experienced the best outcomes received NK cells grown from umbilical-cord blood that was frozen within 24 hours of collection and lacked nucleated red blood cells, an indicator of physical stress. For those who received NK cells from such optimal cord-blood units, the one-year survival rate was 69%. When the cord blood did not meet these standards, it was just 5%. “The minute we came up with this, we went and changed all of our protocols,” Rezvani says — now she uses only optimal cord blood.
Rezvani says that her team is constantly incorporating ideas from NK-cell-biology research into its efforts to use the cells in treatment. This includes methods of processing NK cells that don’t involve any genetic engineering and that improve the cells’ function in the body. About 15 years ago, for example, researchers at Washington University School of Medicine found that a particular blend of cytokines could reprogram mouse NK cells to become more easily activated when they are stimulated for a second time. The cells retained this memory-like quality weeks after being injected into different mice7.
Working in Fehniger’s lab, immunologist Rizwan Romee, who is now a medical oncologist at the Dana-Farber Cancer Institute in Boston, Massachusetts, and his colleagues found that it was possible to nudge human NK cells into a similar memory-like state in which the cells live longer, divide more, make more pro-inflammatory cytokines and resist inhibitory signals. The team first tested the cells in nine people with acute myeloid leukaemia (AML), and found that the cells cleared the cancer in five people — one of whom had been through four previous failed therapies8. This was encouraging, Romee says, because AML is notoriously difficult to treat and T-cell therapies have made little headway against it. NK cells, by contrast, naturally recognize AML cells well. “This is where NK cells should shine, based on their biology,” Romee says.
Fehniger and his colleagues are testing memory-like NK cells as an add-on therapy to stem-cell transplantation in adults and children with AML. In experiments in which the NK cells came from the same donor, the cells multiplied 1,000-fold and lasted for at least 2 months9. His team is also detailing the characteristics that distinguish memory-like NK cells using tools such as mass cytometry, which can measure dozens of proteins or genes in millions of individual cells at a time. In 2021, the biotechnology company Wugen, which is based in St Louis and was co-founded by Fehniger, obtained the licence for the memory-like NK-cell protocol. Wugen is now testing its own cryopreserved off-the-shelf NK-cell product in people with AML and some solid tumours.
A post-treatment tumour biopsy shows active natural killer cells (white).Credit: Ref. 10
Romee, meanwhile, has started an NK-cell programme at Dana-Farber. He and his colleagues are testing memory-like NK cells against AML and other cancers, and engineering the cells with cancer-targeting CARs.
Researchers are continuing to explore pre-treatment ‘recipes’ that could boost NK-cell function once the cells have been transferred into the body. In the past year, the biotechnology company Gamida Cell, which is based in both Boston and Kiryat Gat, Israel, have identified multiple benefits of growing NK cells with IL-15 and nicotinamide — a water-soluble form of vitamin B10. The combination improves the metabolism of NK cells, protects them from oxidative stress, enhances their cancer-killing activity and turns on genes for surface proteins that improve their ability to home in on tumour sites.
Veronika Bachanova, an oncologist at the University of Minnesota Medical School in Minneapolis, partnered with Gamida Cell to examine the effects of nicotinamide on NK cells and test them in a phase I trial in combination with rituximab, a monoclonal antibody that targets B-cell cancers. In a study published last year, the researchers showed that 13 out of 19 people with advanced non-Hodgkin’s lymphoma responded to the combination10. A lymph-node biopsy from one person showed that the treatment encouraged T cells to infiltrate the cancerous tissue. So, even though the NK cells might be around for only a couple of weeks, Bachanova says, that might be enough to stimulate a powerful anti-cancer immune response. Gamida Cell is continuing this work in a phase II trial.
By combining NK cells with rituximab, the biotech firm is one of many companies taking advantage of a natural interaction between antibodies and the potent NK-cell activating receptor, CD16. “We are actually using the antibody for the targeting,” says Fred Aslan, chief executive of Artiva Biotherapeutics in San Diego, California, which is also testing this combination. “We have the luxury of not having to engineer our product because it naturally will kill the [cancer] cells once they are tagged by the antibody.” Aslan says that Artiva has enhanced the effect by using only NK cells from umbilical-cord blood donors who have a naturally occurring CD16 variant that binds extra tightly to antibodies.
Initial results from a phase I trial showed that Artiva’s combination shrank or eliminated signs of tumours in four out of six people with non-Hodgkin’s lymphoma — three of whom had previously undergone CAR-T therapy without success11. As far as the issue of persistence is concerned, Aslan says, the team’s remedy is simply to give people high doses of NK cells, which is possible because of their safety. “NK cells are not really designed to be one-and-done like CAR-T cells, in terms of their expansion,” he says. He hopes that updated results from the non-Hodgkin’s lymphoma trial, expected later this year, will help to make the case that, at the right doses, even unedited NK cells can produce lasting remission.
Working with what you’ve got
Because of their multitude of cancer-detecting receptors, NK cells that are already present in the body are becoming a popular target for drugs that aim to activate anti-tumour immunity. In fact, for many types of cancer, an abundance of NK cells in a tumour is linked to a better outcome. The problem is that tumours can disarm NK cells by, for example, triggering inhibitory receptors or producing enzymes that snip off activating receptors such as CD16. NK cells are also sensitive to nutrient competition and metabolic stress, which are common in tumour microenvironments.
“The tumour microenvironment is a challenging environment for NK cells to operate in,” says Nicholas Huntington, a cancer immunologist at Monash University in Melbourne, Australia. “We’re looking at ways of improving their metabolism, fitness and function so we can restore some of that innate natural killing ability.” Huntington is a co-founder of oNKo-innate, a company in Melbourne focused on finding targets for small-molecule drugs that could enhance NK-cell function. One of its drug candidates, for example, enhances NK-cell and T-cell sensitivity to IL-15.
Others are taking advantage of known activating and inhibitory receptors to bolster existing NK cells. Innate Pharma, a biotechnology firm based in Marseille, France, is testing an NK-cell checkpoint inhibitor in a phase III trial as a complement to T-cell checkpoint-inhibitor therapy for non-small-cell lung cancer. The drug blocks an inhibitory receptor found on NK cells and some T cells called NKG2A, unleashing both branches of the immune response.
More from Nature Outlooks
Innate Pharma has also designed a suite of molecules called engagers, which simultaneously activate immune cells and bring them into close proximity to their targets by binding known tumour antigens. Engagers that bind T-cell receptors are already in clinical use, but they carry a high risk of cytokine release syndrome. NK-cell engagers pose a safer alternative that could still ignite anti-cancer immunity. The company’s tri-specific engager binds to blood-cancer proteins, CD16 and another NK-activating receptor; its tetra-specific engager has an added region that stimulates the IL-2 receptor on NK cells, but not on Treg cells. In mouse studies, the tetra-specific engager caused NK cells to infiltrate solid lung tumours12, a feat that has been difficult in immunotherapy.
Researchers have started pairing engagers with NK cells to get the most from both therapies. Last year, Rezvani and her colleagues reported their findings on a CD16-based engager made by Affimed, a pharmaceutical firm in Mannheim, Germany, in combination with cord-blood-derived memory-like NK cells. The trial tested different doses of cells in people with blood cancer, most of whom had chemotherapy-resistant Hodgkin’s lymphoma and had already been through an average of seven lines of therapy. Of the 36 people who were given the highest dose of NK cells plus the engager, 72% experienced complete remission13.
Aslan says that Artiva is testing Affimed’s engager with its NK cells in a phase I/II trial designed to gather the data needed to apply for FDA approval if the results are good. Fehniger expects the first regulatory approval for NK-cell therapy to come in the next several years. “There are a lot of examples where we’re really close,” he says.
For Bachanova, the work and the wait are well worth it on the basis of the remissions she has seen over the years that avoid the intense side effects common with T-cell therapies. “The patients feel good,” she says. “You witness that and it is powerful.”
Lurking throughout your body, from your liver to your brain, are zombie-like entities known as senescent cells. They no longer divide or function as they once did, yet they resist death and spew out a noxious brew of biological signals that can slow cognition, increase frailty and weaken the immune system. Worst of all, their numbers increase as you age.
For more than a decade, researchers have been trying to see whether they can selectively destroy these cells with a variety of drugs. In a pivotal study1 published in 2015, a team at the Mayo Clinic in Rochester, Minnesota, and at the Scripps Research Institute in Jupiter, Florida, discovered that a combination of two compounds, called dasatinib and quercetin, killed senescent cells in aged mice. The treatment made the mice less frail, rejuvenated their hearts and boosted their running endurance. The finding opened the door to a new area of medicine called senolytics.
Now, fresh results from animal studies and human clinical trials have added momentum to the field. In mice and monkeys, researchers are using genetic tools to reprogram and kill senescent cells. Others are engineering senolytic immune cells. And about 20 clinical trials are ongoing. Researchers are testing new and repurposed drugs that could have senolytic properties, in the hope of combating age-related conditions, including Alzheimer’s disease, lung disease and chronic kidney disease.
“I am convinced that senolytics will have an impact in the clinic,” says Anirvan Ghosh, chief executive of Unity Biotechnology, a company in South San Francisco, California, that is developing senolytics. “I think the question is really what the agent looks like and what the first approved drug is.”
Zombie cells
Senescent cells were first described in 1961 by US biologists Leonard Hayflick and Paul Moorhead, who discovered that human cells in a laboratory dish will divide no more than about 50 times before either dying or entering the twilight state of cell senescence2. In the lab, it can take weeks for dividing cells to become senescent. But researchers have yet to uncover how much time this process takes in the body, how long senescent cells last and whether all cell types can become senescent.
Hacking the immune system could slow ageing — here’s how
Beyond hitting the limits of cell division, cell senescence can arise owing to other factors such as physical injury, malnourishment or DNA damage caused by UV light. Researchers initially thought that it evolved to prevent damaged cells from replicating uncontrollably and causing cancer. This might be the case to some extent, but it didn’t make sense that the cells would stick around in the body instead of simply dying, such as through the controlled programme of cell death known as apoptosis.
Researchers eventually discovered that senescent cells were avoiding apoptosis so they could perform a service, belching out a potent mix of inflammatory signals — including the cytokines interleukin-6 and interferon-γ — that prompt the immune system to clear out damaged cells. This helps to make room for damaged tissues to regenerate and repair.
The process works well until the immune system weakens with age, leading to a build-up of senescent cells that stir up excessive inflammation. Researchers have found that an accumulation of senescent cells and age-related inflammation correlates with many diseases, including osteoporosis, diabetes, heart disease, kidney disease and Alzheimer’s disease. For many scientists in the field, this realization prompted a shift away from understanding what the cells are doing to working out how to kill them.
Tipping the balance
One key strategy in senolytics involves designing drugs that stop senescent cells from resisting apoptosis. Usually, the cells survive by producing anti-death proteins. Blocking these with drugs can force the cells to succumb to death.
Unity Biotechnology is at the forefront of this approach, say researchers. In a February study3, Ghosh and his colleagues found that senescent cells were more abundant in the retinas of diabetic mice than in those of healthy mice. It was possible, the team predicted, that senescent cells in the blood vessels of the eye play a part in diabetes-related vision loss.
Why is exercise good for you? Scientists are finding answers in our cells
This condition, known as diabetic macular oedema, is caused by high blood sugar and makes those delicate blood vessels leaky, particularly in older individuals. The eye condition is a leading cause of blindness worldwide, estimated to affect 27 million adults. But around half of patients get little benefit from the standard treatment, which uses a cancer drug originally designed to slow down the growth of blood vessels. “There is an unmet need,” Ghosh says.
The researchers designed a drug, called foselutoclax, which blocks the action of BCL-xL, a key anti-death protein that is abundant in senescent cells. When they injected the drug into the eyes of diabetic mice, it killed senescent cells in the blood vessels supplying the retina, but not healthy cells3. “We see a very selective elimination,” says Ghosh.
The senolytic drug reduced the leakiness of retinal blood vessels in diabetic mice by around 50%. Moreover, the treated mice performed better in vision tests compared with controls. Next, the team turned to humans. In a phase II trial, researchers administered a single injection of foselutoclax into the eyes of about 30 people. Eleven months later, those treated with the senolytic could read 5.6 more letters, on average, on an optician’s chart compared with participants who had received a placebo treatment.
After just a couple of weeks, says Ghosh, one participant called him to say the treatment was making her life much easier. Another saw rapid improvements in their colour vision. The team expects to publish the results later this year, but in the meantime, Unity is running another phase II trial that will compare the senolytic with standard therapy.
Unity’s results are promising, say researchers. “I think within the next five years we may see this treatment for diabetic macular oedema being offered in the clinic,” says Sundeep Khosla, who studies ageing at the Mayo Clinic.
Rather than making senolytics from scratch, some scientists are testing drugs that already exist. These include dasatinib, which is approved in the United States as a cancer therapy, and two commercially available, plant-derived chemicals called quercetin and fisetin. The latter two are sold as supplements to dampen inflammation, boost brain health and reduce the risk of age-related disease. These claims are based on rodent studies in which the drugs have been shown to clear senescent cells and reduce inflammation4.
Do cutting-edge CAR-T-cell therapies cause cancer? What the data say
In a 2019 study5, researchers used dasatinib and quercetin to remove senescent brain cells in a mouse model of Alzheimer’s disease. Mice treated with the senolytics had reduced brain inflammation and improved memory compared with animals that were given a placebo. Spurred on by these promising data from mice, Miranda Orr at Wake Forest University School of Medicine in Winston-Salem, North Carolina, and her colleagues last year conducted the first safety trial of the drug combination in people with early stage Alzheimer’s disease.
Orr’s team gave five people dasatinib and quercetin intermittently for three months. The researchers found that the drugs were safe and that dasatinib was present in samples of cerebrospinal fluid, suggesting it could cross into the brain. Quercetin was not detected in brain fluid samples, but Orr says she suspects that it did reach the brain and was rapidly broken down. The team is now conducting a larger trial to track the cognition of people with and without Alzheimer’s disease for nine months after they take a placebo or the drug combination. The results should be released in 2025, says Orr.
Khosla says that fresh data should also emerge this year from the largest human trial of dasatinib and quercetin so far. In this study, which is currently under peer review, his team looked at the effect of senolytics on the bones of healthy women.
Immune killers
When it comes to killing cells in the body, the immune system could be of help. And some researchers have latched on to the idea of using genetically engineered immune cells called chimeric antigen receptor (CAR) T cells. These can target and kill specific cells on the basis of the molecules they display on their surface. CAR-T-cell therapies are currently approved as a treatment for various blood cancers.
Earlier this year, cell biologist Corina Amor at Cold Spring Harbor Laboratory in New York and her colleagues identified a protein marker, called uPAR, on senescent cells in the livers, fat tissues and pancreases of older mice6. The researchers created CAR T cells that were designed to kill senescent cells bearing the uPAR marker. After the team infused the engineered cells into the blood of old mice, there was a decline in the proportion of liver, pancreas and fat cells that were senescent.
Senescent mouse liver cells express β-galactosidase (white) and uPAR (yellow).Credit: Memorial Sloan Kettering Cancer Center
Amor and her team found that old mice treated with the uPAR CAR T cells had reduced blood-sugar levels — a sign of improved metabolic health — and that the animals ran faster and for longer than did mice treated with non-engineered T cells, or with T cells that target a protein not found in mice. None of the mice treated with the senolytic CAR T cells showed signs that the T cells were toxic.
In young mice, the senolytic CAR T cells prevented age-related declines in blood-sugar regulation and exercise capacity. And in a March preprint7, the team reported that senolytic CAR T cells could rejuvenate the guts of old mice.
Still, further studies are needed to assess the safety of the therapy, says Amor. Moreover, it would be good to have an off switch for these cell-based drugs in case anything goes awry, she says. In rare cases, CAR T cells used to treat cancer in people seem to have become cancerous themselves.
Amor’s team plans to explore such safety switches in the near future. This would involve engineering the senolytic CAR T cells to carry a gene that induces cell death, which could be activated with a drug, she says. But CAR-T-cell therapies are expensive to make, says Robin Mansukhani, chief executive of Deciduous Therapeutics in San Francisco, which is also developing immune therapies against ageing.
Mansukhani is banking on a more affordable approach that harnesses a different kind of immune cell called a natural killer T cell. In 2021, researchers at Deciduous Therapeutics demonstrated8 the senolytic role of these cells, which naturally become less effective with age. They also found that drugs that can activate the immune cells helped to eliminate senescent cells in the damaged lungs of mice, reducing lung scarring and improving survival.
The researchers have developed a range of drugs that can bind to and supercharge natural killer T cells to treat various conditions, including diabetes and lung disease, says Mansukhani. Safety tests will be conducted in dogs and non-human primates later this year, and clinical trials should begin in the next two years, Mansukhani adds. The approach relies on smaller molecules that are easier to make than CAR-T-cell therapies, he says.
Gene therapy
Other teams are using gene therapy to kill senescent cells. In this approach, researchers package a gene that encodes a lethal protein called caspase-9 into fatty capsules studded with proteins derived from a virus. In mice and monkeys, the capsules have been found to deliver the gene to cells in the lungs, heart, liver, spleen and kidneys.
To stay young, kill zombie cells
Healthy cells are spared, because the gene is activated only in senescent cells that have high levels of one of two proteins called p16 and p53, says Matthew Scholz, chief executive at Oisín Biotechnologies in Seattle, Washington, which is developing the gene therapy. As a further safety switch, the lethal protein kicks off cell death only after the animal is given a very low dose of a drug called rapamycin, says Scholz. The researchers found that, over four months, a monthly dose of the therapy reduced frailty and cancer rates in old mice without causing harmful side effects. The comparison group involved mice that were given a placebo and low-dose rapamycin, says Scholz.
But a key limitation of this approach is that it relies on just one or two protein markers. Although p16 is widely used as a marker of senescence, definitive identification of cells in this state requires a panel of several markers. That means that, by targeting only p16 and p53, the gene therapy is probably eliminating some healthy, non-senescent cells that have these markers, and failing to kill some senescent cells that lack them, say researchers.
Better markers
Indeed, the issue of specificity is shared by all senolytic approaches, simply because there is more than one type of senescent cell. Researchers are only just beginning to uncover how many there are — and what markers they bear. “Without having really great biomarkers of senescent cells, it’s a little bit tricky to engage the right targets,” says Orr.
Orr is part of a large collaborative effort called the Cellular Senescence Network (SenNet), involving more than 200 researchers, that aims to produce atlases of senescent cells across the lifespan of humans and mice. Her team is using machine learning to improve definitions of brain-cell markers of senescence, then using them to map how senescent cells change with age and during dementia.
Ultimately, better markers of senescent cells will bring better senolytics that could one day prevent or treat age-related disease, she says. Ghosh echoes this optimism when it comes to killing zombie cells. “I think the fundamental science is so compelling that targeting senescent cells is definitely going to be of benefit.”
Stem-cell researcher Carolina Florian didn’t trust what she was seeing. Her elderly laboratory mice were starting to look younger. They were more sprightly and their coats were sleeker. Yet all she had done was to briefly treat them — many weeks earlier — with a drug that corrected the organization of proteins inside a type of stem cell.
When technicians who were replicating her experiment in two other labs found the same thing, she started to feel more confident that the treatment was somehow rejuvenating the animals. In two papers, in 2020 and 2022, her team described how the approach extends the lifespan of mice and keeps them fit into old age1,2.
The target of Florian’s elixir is the immune system. The stem cells she treated are called haematopoietic, or blood, stem cells (HS cells), which give rise to all immune cells. As blood circulates, the mix of cells pervades every organ, affecting all bodily functions.
But the molecular composition of the HS cells changes with age, and this distorts the balance of immune cells that they produce. “Fixing the drift in them that occurs with time seems to fix a lot of the problems of ageing — not only in the immune system but also in the rest of the body,” says Florian, who is now at the Bellvitge Biomedical Research Institute in Barcelona, Spain.
In March3, another team showed that restoring the balance between two key types of immune cell gives old mice more youthful immune systems, improving the animals’ ability to respond to vaccines and to stave off viral infections.
How to make an old immune system young again
Other scientists have used different experimental approaches to draw the same conclusion: rejuvenating the immune system rejuvenates many organs in an animal’s body, at least in mice. And, most intriguingly, evidence suggests that immune-system ageing might actually drive the ageing of those organs.
The potential — helping people to remain healthy in their later years — is seductive. But translating this knowledge into the clinic will be challenging. Interfering with the highly complex immune system can be perilous, researchers warn. So, at first, pioneers are setting their sights on important yet low-risk goals such as improving older people’s responses to vaccinations and improving the efficiency of cancer immunotherapies.
“The prospect that reversing immune ageing may control age-related diseases is enticing,” says stem-cell scientist Vittorio Sebastiano at Stanford Medical School in California. “But we are moving forward cautiously.”
Fading immunity
The human immune system is a complex beast whose multitudinous cellular and molecular components work together to shape development, protect against infections, help wounds to heal and eliminate cells that threaten to become cancerous. But it becomes less effective as people age and the system’s composition starts to change. In older age, people become susceptible to a range of infectious and non-infectious diseases — and more resistant to the protective power of vaccines.
The immune system has two main components: a fast-acting innate system, which destroys invading pathogens indiscriminately, and a more-precise adaptive immune system, whose components learn to recognize specific foreign bacteria and viruses and generate antibodies against them.
The HS cells in the bone marrow spawn the immune cells of both arms of the system. They differentiate into two main classes — lymphoid and myeloid — which go on to differentiate further. Lymphoid cells are mostly responsible for adaptive immunity, and include: B cells, which produce antibodies; T cells, which help to attack invaders and orchestrate complex immune responses; and natural killer cells, which destroy infected cells. Myeloid cells include a raft of cell types involved mostly in innate immunity.
Proteins inside immune-cell-generating stem cells become more symmetrical with age (right).Credit: Eva Mejia-Ramirez
One of the earliest changes in the immune system as people age is the shrinking of the thymus, which begins after puberty. This organ is the crucible for T cells, but a lot of the tissue has turned to fat by the time people hit their 30s, slashing the production of new T cells and diminishing the power of the immune system. What’s more, the function of T cells alters as they age and become less specialized in their ability to recognize infectious agents.
The proportions of different types of immune cell circulating in the blood also changes. The ratio of myeloid to lymphoid cells skews markedly towards myeloid cells, which can drive inflammation. Moreover, increasing numbers of immune cells become senescent, meaning that they stop replicating but don’t die.
Any cell in the body can become senescent, typically when damaged by a mutation. Once in this state, cells start to secrete inflammatory signals, flagging themselves for destruction. This is an important anticancer and wound-healing mechanism that works well in youth. But when too much damage accumulates with ageing — and immune cells themselves also become senescent — the mechanism breaks down. Senescent immune cells, attracted by the inflammatory signals from senescent tissue, secrete their own inflammatory molecules. So not only do they fail to clean up properly, but they also add to the inflammation that damages surrounding healthy tissue. The phenomenon is known as ‘inflammaging’.
“It becomes a terrible positive feedback — a never-ending dance of destruction,” says immunologist Arne Akbar at University College London.
And evidence suggests that this feedback loop is kicked off by the immune system. In a series of experiments in mice4, Laura Niedernhofer at the University of Minnesota in Minneapolis has shown that immune-cell senescence actually drives senescence in other tissues. “These cells are extremely dangerous,” she says.
Her team used genetic methods to eliminate an important DNA-repair enzyme in the immune system of the mice. The animals remained healthy until adulthood but then, unable to correct accumulating mutations, various types of immune cell started to become senescent.
A few months later, increasing numbers of cells in organs such as the liver and kidney also fell into senescence, and the organs showed signs of damage. These effects were all reversed when the scientists gave the mice immune cells from the spleens of young, healthy mice.
All of this suggests that fixing the characteristics of immune-system ageing could help to prevent or mitigate diseases of ageing, says Niedernhofer.
Battling senescence
Many scientists are trying to do just that, from very different angles. Lots of the approaches hint that very short treatments of the immune system might have long-term effects, keeping side effects to a more manageable minimum.
One approach is to tackle senescent immune cells head on, using drugs to either remove them or block the inflammatory factors they secrete. “Senescent immune cells have long been known to be very modifiable in humans,” says Niedernhofer. “They go up if you smoke and down if you exercise.”
Are your organs ageing well? The blood holds clues
Some drugs — such as dasatinib, which is approved for the treatment of some cancers, and quercetin, which is marketed as an antioxidant dietary supplement but not approved as a drug — are known to reduce the age-related acceleration of senescence, and dozens of clinical trials are testing their impact on various age-related diseases. Niedernhofer herself is involved in a small clinical trial on older people with sepsis, a condition that becomes more deadly with age.
Her team is also doing experiments to assess which of the many types of immune cell is the most important in driving senescence in the body, which should help in the design of more precise therapies. Two types — T cells and natural killer cells — are emerging as key contenders, she says. She plans to screen natural products and drugs already approved for use by the US Food and Drug Administration for their ability to interact with those types of immune cell in senescence.
Akbar thinks that targeting inflammation itself might be as effective as targeting the senescent cells. He and his colleagues did a study in healthy volunteers using the investigational compound losmapimod, which blocks an enzyme involved in the production of inflammatory molecules called cytokines. They treated the volunteers with the drug for four days, and then, over the course of a week, measured their skin responses to an injection of the virus that causes chickenpox. Most people are exposed to this virus during their lives and it frequently lingers in the body. But with age, people tend to lose their immunity to it, and it can then manifest as shingles. The drug restored the immune response in the skin in older volunteers to a level similar to that seen in the younger volunteers5. In unpublished work, Akbar has found the same robust skin results up to three months later.
“Temporarily blocking inflammation in this way to allow the immune system to function might similarly boost the response of older patients to flu vaccinations,” says Akbar.
Immune boost
The value of priming the aged immune system before administering a vaccine has been demonstrated in a series of clinical trials led by researcher Joan Mannick, chief executive of Tornado Therapeutics, which is headquartered in Boston, Massachusetts. Those trials tested analogues of the drug rapamycin and other drugs with similar mechanisms, which target the immune system and are approved for prevention of organ transplant rejection and for the treatment of some cancers. The drugs block an enzyme, called mTOR, that is crucial for many physiological functions and which becomes dysregulated in old age.
For several weeks before receiving their influenza vaccinations, trial participants were treated with doses of the drugs that were low enough to avoid side effects. This treatment regimen improved their responses to the vaccine, and boosted the ability of their immune systems to resist viral infections in general.
Vaccines tend to work less efficiently in older adults, but new approaches could boost their power.Credit: Hector Vivas/Getty
But rapamycin can raise susceptibility to infection and affect metabolism, so Mannick is planning trials with similar drugs that might have a safer profile. “But there are all sorts of different ways to try to improve the immune system,” she notes.
One other way is to try to restore the function of the thymus to maintain the production of new T cells. Immunologist Jarrod Dudakov at the Fred Hutchinson Cancer Center in Seattle, Washington, is researching the basic biology of thymus cells to try to work out how they regenerate themselves after stressful assaults. “It’s all a bit early to see how this understanding will translate into the clinic,” he says. But he thinks that maintaining the ability of the thymus to generate a broad repertoire of T cells will be “foundational”.
Others are trying to combat ageing by generating thymic tissue from pluripotent stem cells for eventual transplantation. But Greg Fahy, chief scientific officer at Intervene Immune in Torrance, California, says he sees no need to wait for these long-term prospects to come to fruition, because an available drug — synthetic growth hormone — is already known to regenerate thymus tissue. He is doing a series of small studies on healthy volunteers using growth hormone as part of a cocktail of compounds. Early results indicate that the participants show increased levels of functional thymic tissue, and that their epigenetic clock — a biomarker of ageing — reverses by a couple of years6. Fahy is now extending the trial to look at whether the drug cocktail also improves physical fitness in a larger group of volunteers.
Turn back time
Another approach, not yet in the clinic, is to partially reprogram immune cells, to try to turn back the clock in cells that have become senescent. This involves transiently exposing the cells in a dish to a cocktail of transcription factors known to induce a pluripotent state in adult cells.
Reversal of biological clock restores vision in old mice
Sebastiano and his colleagues have shown in human cells that this process corrects the epigenetic changes that occur with ageing7. He has co-founded a start-up company to use the technique to try to counteract a problem in a cancer therapy known as CAR T, in which T cells are engineered outside the body to target and destroy a person’s cancer. But the T cells can turn senescent before they can be returned to the person. Rejuvenating them during the generation process would make production quicker and more robust, says Sebastiano.
Florian’s approach, too, aims to produce healthier immune cells — inside the body1,2. HS cells in the blood rack up epigenetic changes, and their environment also changes as they age. This causes proteins in the cells to arrange themselves more symmetrically — a process known as polarization — which shifts the balance of stem-cell differentiation in favour of myeloid cells over lymphoid cells. Florian’s studies used a four-day treatment with a compound, called CASIN, that inhibits one part of this process to correct the polarization, and helped the mice to live longer.
The team saw the same life-extending effects when HS cells from old mice given CASIN were transplanted into old mice that hadn’t received the treatment. “This very small step had a large impact,” says Florian.
Florian next hopes to bring her work to the clinic. As a first case study, she thinks her drug might support regeneration of the immune system after people receive chemotherapy for cancer.
How old?
Research on immune ageing faces some fundamental challenges. One is shared with ageing studies in all organs — the inability to measure ageing precisely.
“We don’t know in a quantitative, measurable, predictive way what ageing means at the molecular level in different cell types,” says Sebastiano. “Without those benchmarks, it is very hard to show rejuvenation.” Last year, a consortium of academics got together to begin developing a consensus on biomarkers of ageing — which will be essential when scientists come to seek approval from regulatory agencies for anti-ageing therapies.
Another challenge is the difficulty in pinning down what makes one immune cell unique. Until recently, it has been hard to demonstrate which subtypes of immune cells live where, and how they change with time.
But technologies such as single-cell RNA sequencing, which quantitatively measures the genes being expressed in individual cells, have tightened up analysis. A large study of immune cells in the blood of mice and humans across a range of ages published last November, for example, revealed 55 subpopulations. Just twelve of those changed with age8.
With so many strands of research coming together, scientists are cautiously hopeful that the immune system will indeed prove to be a key lever in healthy ageing. Don’t expect an elixir of youth any time soon, says Florian — by definition, ageing research takes a long time. “But there is such great potential for translation.”
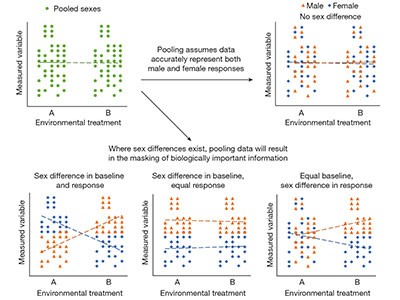
Female animals and women have been ignored or actively excluded in clinical and laboratory-based biomedical research since such research began. This was especially true until the US Congress passed the National Institutes of Health (NIH) Revitalization Act in 1993, which directed the NIH to establish guidelines on the inclusion of women and members of under-represented racial and ethnic groups in clinical trials.
By 2009, a review of 10 fields in biology found that more than 60% of studies with human participants reported on both sexes. For studies using non-human animals, however, only 26% included both male and female subjects1.
To try to correct this persistent imbalance, the NIH implemented extra guidelines in 2016 — this time, on the inclusion of sex as a biological variable in all preclinical research2. At least with respect to the inclusion of female individuals in basic research, this funding-agency mandate and others like it have been effective. Another bibliometric analysis found that 49% of 720 studies on animals published in 2019 used both males and females3.
Why it’s essential to study sex and gender, even as tensions rise
Although it is still early days and there is much room for improvement, the inclusion of female participants and animal subjects is already having a revolutionary impact on numerous areas of study — from chronic pain to mental health. Yet we see an impending collision between research policies and societal changes regarding ideas and attitudes around sex and gender that threatens this nascent enterprise. We also see the threat of lobbyists, legislators and others in the United States and elsewhere weaponizing research on sex differences — either to marginalize individuals or groups that they deem to be outside a narrowly defined norm, or to reinforce derogatory ideas about people who identify as divergent4. (In this article, sex refers to differences between females and males caused by biological factors, whereas gender refers to differences caused by social factors, including gender roles, expectations and identity.)
Our concern is that various critiques of research on sex differences from scholars approaching sex and gender from different viewpoints — in combination with valid concerns around the misinterpretation or misuse of findings — could undermine an approach that has proved both practical and powerful. As a counterweight to this possibility, here we argue for the ongoing value of comparing female and male individuals in biomedical research.
Mammalian biology
Several scholars have argued in recent years that an overemphasis on biological sex will distract investigators from the effects of gendered environments and of non-sex-related variables, such as age, ethnicity or socio-economic status, on many traits. Another common criticism is that comparing female and male participants ignores transgender people and other individuals who do not fall within these binary categories, leading to their further marginalization in society5. Others have argued that a focus on the difference between the mean values of male and female individuals distracts researchers from considering the variability around those means — the implication being that variability within a sex is more important than variability between sexes. Some even question whether sex is a viable concept6.
Before addressing these specific complaints, it is worth briefly reviewing the current understanding of mammalian biology as it relates to sex — as well as some of the diverse and surprising findings that have already emerged from research comparing two sexes.
We need more-nuanced approaches to exploring sex and gender in research
Sex has been with us since our species originated as a result of sexual reproduction. The division of humans and other mammals into two sexes, female and male, derives from the fact that each individual is created by the union of a sperm and an egg. On the basis of the type of germ cell (gamete) that reproducing individuals are able to produce, there are only two sex categories in mammals. (Intersex is not a third category with respect to the type of gamete individuals can produce.) Indeed, understanding of how the mammalian genome evolved and how it functions is based on the foundation of sexual reproduction.
In mammals, as in many other taxa, the biological difference between sexes starts with the genetic difference encoded by the sex chromosomes — typically XX and XY in mammals — which are the only features that differ in female and male zygotes at the beginning of life. The salient role of the sex chromosomes is determining whether the embryo will develop ovaries or testes, because this specifies the type of germ cell that will be made, and the level and secretory patterns of testicular or ovarian hormones. Sex-chromosome genes and gonadal hormones influence almost every tissue in the body. The result might be sex differences in tissue development and function, or similar phenotypes based on different underlying mechanisms7.
Sex differences in immune function might have arisen from the need for female organisms to transfer immunity to the next generation.Credit: Klein & Hubert/Nature Picture Library
As in all things in biology, in humans and other mammals there are variations in the number and type of sex chromosomes and in the downstream mechanisms determining the phenotypic features associated with sex. This leads to variability among individuals in diverse sex-related traits, such as genital anatomy, body size and some behaviours. Also, particularly in humans, biological factors that drive sex differences in cells and tissues are confounded by social and environmental factors that also cause differences between individuals.
To serve all individuals equitably — including those who experience an incongruency between the sex they were assigned at birth and their current gender identity, and those who do not find that they align with either the male or female sex category — the medical profession and biomedical community must identify and interrogate these variations in biological attributes and in lived experiences, all of which can influence people’s physiology, risk of developing disease and prognosis8. This includes carefully attending to the distinctions between cisgender, transgender and non-binary individuals when reporting findings.
Yet we maintain that, in humans and other mammals, the comparison of individuals who have XX chromosomes and ovaries with individuals who have XY chromosomes and testes is a necessary component of basic and clinical research that seeks to improve human health.
Rich pickings
Male and female individuals represent most of the mammalian population. And research regarding biological sex differences has focused first on the largest groups, but in a manner that provides insights about variation within and beyond the binary.
For example, investigators have manipulated factors such as gonadal hormones and sex-chromosome genes to test their effects on sexual differentiation and their role in sex differences in disease. These manipulations, which mimic numerous intersex variations, such as the presence of ovarian hormonal secretions in an individual with XY chromosomes, have shed light on the effects of hormones, sex-chromosome genes and other factors in everyone. Studies of people with a variety of naturally occurring hormonal and chromosomal differences, for instance, are consistent with the interpretation that prenatal exposure to androgens, such as testosterone, is an important component of male psychosocial development9.
Nature journals raise the bar on sex and gender reporting in research
Importantly, the study of female and male individuals, as defined here, establishes a baseline measurement against which to compare findings from those who do not fit into a binary categorization scheme.
Understanding the effects of sex also anchors discussions about how different gendered environments intersect with biological differences, to amplify or mitigate their effects. More than half a century of animal research has been key to developing concepts of mammalian sexual differentiation, because in animals, unlike in humans, researchers can manipulate single genes or molecules to observe their effects on phenotypes. Moreover, although numerous environmental or social effects can be manipulated and studied in animals, such as diet, stress and levels of interaction with other individuals, animals provide useful models of the biological effects of sex in the absence of hard-to-control human gendered variables, such as cultural norms and expectations around child care and work.
The power of comparing female and male individuals in biomedical research is demonstrated most convincingly, however, by the data themselves — as illustrated by four examples from our fields of expertise.
Sex chromosomes versus hormones. Until recently, all of the biological hypotheses proposed to explain the significant sex differences in body weight and metabolism found in humans and animals (including birds and other mammals) were centred on the action of hormones. And extensive research during the twentieth century supported the idea that, in mammals, almost all sex differences in tissues other than the gonads (the organs that produce the gametes) result from the effects of ovarian and testicular hormones.
By the early 2000s, researchers studying gonadal development had created mouse models in which the complement of sex chromosomes could be manipulated in individuals with the same type of gonad10. This meant that investigators could assess whether the sex chromosomes cause differences in phenotypes, even when levels of gonadal hormones are similar7. Studies using the modified mice, while confirming the importance of gonadal hormones in influencing body weight and metabolism, uncovered the effects of sex chromosomes11. Comparable studies have also shown that sex chromosomes have much broader effects on physiology and behaviour than was originally thought10.
Accounting for sex and gender makes for better science
The copy number of an X-linked gene called Kdm5c, for example, contributes to a sex difference found in mice in the metabolism of adipose cells12. Mice with XY chromosomes have one copy of Kdm5c. They also have less body fat than do mice with XX chromosomes, which have two copies of the Kdm5c gene.
Over the past two decades, investigators have found that similar sex-chromosome effects contribute to sex differences in many other physiological systems in mice. And these sex differences, in turn, affect individuals’ likelihood of developing autoimmune conditions, cardiovascular diseases, cancer and developmental defects in the neural tube, the embryonic precursor to the central nervous system. The X-linked gene Kdm6a, for instance, increases the severity of autoimmune disease, and protects against bladder cancer and an Alzheimer’s-like disease in XX mice7. Similarly, the Y-linked gene Uty protects against pulmonary hypertension in mice13. Sex-chromosome genes also affect mouse behaviour, from the social behaviour of juveniles to responses to pain, as well as the size of certain brain regions7,10.
All of this work in mice provides investigators with clues about where to look for potential therapeutic targets in the human genome, for diseases that tend to affect women and men differently.
Pain. It is well established that among people with chronic pain, women far outnumber men14. Also, in experimental settings, women tend to be more sensitive than men are to pain — induced, for instance, by the application of heat, cold or pressure.
Pain researchers have proposed various gender-based and sex-based explanations for these differences14, such as that women are more likely than men to go to the doctor, as shown by usage rates for health-care services. However, investigations in male and female mice have suggested that, at least in rodents, different mechanisms are responsible for the processing of persistent pain in females and males.
Why the sexes don’t feel pain the same way
A 2015 study in mice15, for example, and follow-up findings demonstrated that a well-studied mechanism for the processing of persistent pain — involving immune cells called microglia — operates only in male rodents. (It is well studied in males, at least.) In males, the microglia release a factor that causes neurons in the spinal cord to increase their firing, which sustains chronic pain. Although female mice have just as many microglia as male mice do, their microglia don’t seem to be involved in the pain circuit — or, if they are involved, it is in a more complicated way. In fact, in females, T cells might play a similar part to microglia in males.
Whether the microglial or T-cell mechanism for the processing of persistent pain is engaged in any one individual seems to be due to testosterone levels being above or below a certain threshold. This dimorphism suggests that different physiological mechanisms could contribute to some of the differences observed in men and women in relation to chronic pain.
Immune function. Numerous studies that involve comparing immune responses in female and male organisms — whether they are fruit flies, fish, lizards, birds or mammals — have shown that females often generate more robust immune responses to antigens than do their male counterparts16. This suggests that sex differences in immune function are evolutionarily conserved, perhaps because of a common need for female individuals to transfer immunity to the next generation (whether through breast milk or a yolk sac), or because of some other sex-specific selective pressure.
In humans, these immunological stimuli can be self-antigens (proteins made by our own cells), allergens, cancerous cells or pathogenic microbes. Because women have larger immune responses than men, they are more likely to develop autoimmune diseases and allergies, but less likely to be diagnosed with non-reproductive cancers, such as skin or colon cancer17, and certain infectious diseases, such as tuberculosis16 and COVID-1918.
Some studies suggest that women generate a greater immune response to certain vaccines than do men.Credit: Patrick Meinhardt/Bloomberg/Getty
The difference between female and male organisms in the amount of antibodies produced in response to immunological stimuli changes across the life course, being most robust during the reproductive years19. This could explain why females of reproductive age often generate more antibodies in response to vaccines and microbes than males do20, and why female antibody responses are more durable and cross-reactive against diverse variants, such as different strains of influenza virus.
Mouse models have shown that gonadal hormones contribute more to mammalian sex differences in vaccine-induced immunity than do genes linked to sex chromosomes, at least against influenza viruses21. In both mice and humans, concentrations of estradiol (a hormone that is typically produced at higher levels in female organisms) are positively associated with greater antibody responses to influenza vaccines22. In short, a wealth of insights about the benefits (and downsides) of a bolstered immune response have emerged only because researchers have compared immune responses in male and female organisms.
Mental health. Sex and gender differences in the prevalence of mental-health disorders in humans span the life course. Prepubescent boys are significantly more likely than prepubescent girls to be diagnosed with autism spectrum disorder or attention deficit and hyperactivity disorder23. In their late teens or early 20s, men are more likely to be diagnosed with early-life schizophrenia. They are also more likely to experience a brain injury caused by a lack of oxygen at birth, and to have neurological conditions, such as Tourette’s syndrome. After puberty, however, disorders involving depression, anxiety, compulsion and obsession are more frequent in women23.
Sociocultural factors probably contribute to the differences in the prevalence of many of these conditions, including biases around the criteria used to diagnose early-life disorders by clinicians. Similarly, by the time a woman is diagnosed with a mood or affective disorder, she has often lived for decades in a gendered environment, making it hard for researchers to separate the effects of biology during development from those of life experience. Studies conducted over the past two decades in male and female rodents, however, have revealed an integral role for the immune system — specifically microglial cells — in affecting how testosterone acts on the brain and alters the structure and function of certain regions.
The fraught quest to account for sex in biology research
For instance, experiments measuring cellular activity in post-mortem animals have shown that during development, male rodents have a greater number of activated microglia in certain regions of their brains than do female rodents. These activated microglia release more of the signalling molecules that are crucial to forming synapses and controlling cell numbers. Many of the brain regions affected by the selective elimination of cells are also those implicated in mental-health disorders in humans (in both sexes) that originate during development24.
These findings could offer clues as to why messenger RNAs obtained from the cortex of human male fetuses indicate higher expression levels of genes involved in inflammation than do those obtained from human female fetuses. Post-mortem, higher levels of inflammation have even been found in the cortices of men who had been diagnosed with autism than in those of men who had not received a mental-health diagnosis25.
All of this suggests that, in mammals, greater activity of the neuroimmune system is somehow involved in the process of brain masculinization — which means that various mental-health disorders that affect boys more than girls could involve disruptions to immune-system processes.
Early days
Ultimately, we support efforts to interrogate both biological and social determinants of disease. Indeed, having more information is always preferable to having less. It is crucial to consider how biological factors linked to sex interact with each other and with other biological factors, such as age and genetic background, as well as with sociocultural or environmental influences. But whether the variables that have the most impact on physiology and disease are sex-based, gender-based or unrelated to either is a question that must be answered by research.
Sex and gender analysis improves science and engineering
Related to this, although there is always a danger of scientists and journalists oversimplifying things — particularly in relation to sex and gender — any rigorous analysis requires the consideration of averages as well as measures of variation. Just as with the importance of sex-related variables compared to other variables, it is an empirical question whether within-sex variation has more or less impact on a trait of interest than between-sex variation does.
When it comes to the threat of people misusing statements about an inherent difference between female and male individuals to rationalize continuing the historical subordination of women, transgender people and others, we agree that this danger is real and urgent. Since September 2023, for instance, health-care providers in Texas have been prohibited from giving gender-transition surgeries, puberty-blocking medication or hormone therapies to people under 18. This was decided on the basis of claims that everyone belongs to one of two groups, and that this reality is settled by science. The solution, however, is not to deny a priori the importance of sex differences, but rather to improve understanding of variation in human populations and how it relates to biological and social factors. Similarly, whereas we recognize the importance of studying intersex, non-binary, transgender and other individuals whose biology or life experiences are not encompassed by a simplistic binary, the neglect of such individuals should not be addressed by abandoning female–male comparisons.
Because female organisms have for so long been left out of investigations in many biomedical fields, researchers are still surprisingly ignorant of their fundamental biology across numerous taxa, and how it does or does not differ from that of males. There is also much room for improvement in research on sex differences — in terms of statistical and reporting practices26, researchers actually splitting their data by sex and analysing those data appropriately3, and journals improving their policies around sex and gender. The highly fruitful approach of comparing female and male organisms should not be abandoned just as investigators are starting to make progress.
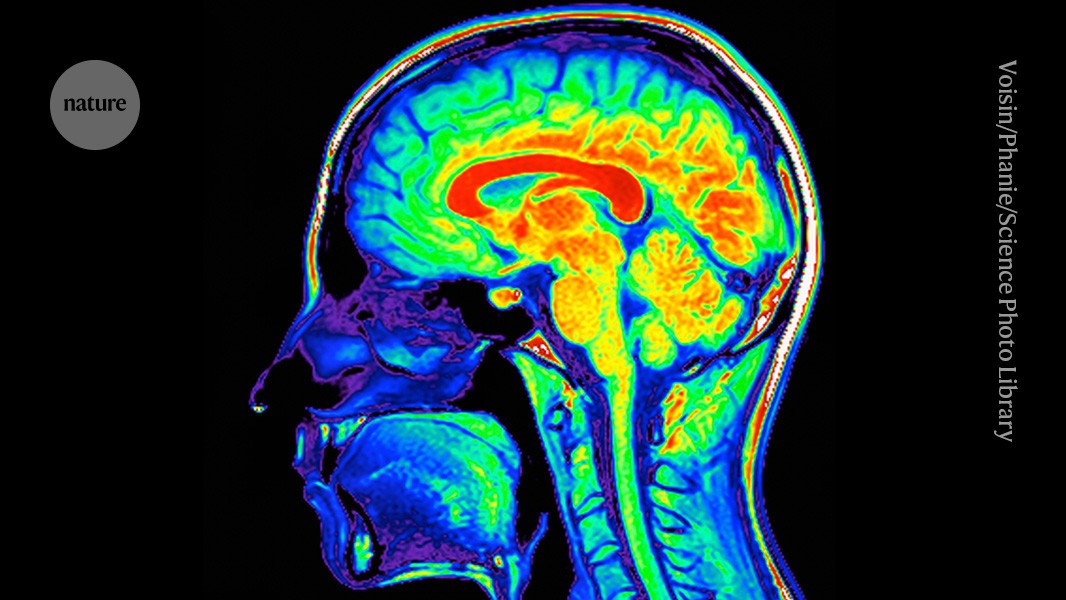
A population of neurons in the brain stem, the stalk-like structure that connects the bulk of the brain to the spinal cord, acts as the master dial for the immune system.Credit: Voisin/Phanie/Science Photo Library
Scientists have long known that the brain plays a part in the immune system — but how it does so has been a mystery. Now, scientists have identified cells in the brainstem that sense immune cues from the periphery of the body and act as master regulators of the body’s inflammatory response.
The results, published on 1 May in Nature1, suggest that the brain maintains a delicate balance between the molecular signals that promote inflammation and those that dampen it — a finding that could lead to treatments for autoimmune diseases and other conditions caused by an excessive immune response.
The discovery is akin to a black-swan event — unexpected but making perfect sense once revealed, says Ruslan Medzhitov, an immunologist at Yale University in New Haven, Connecticut. Scientists have known that the brainstem has many functions, such as controlling basic processes such as breathing. However, he adds, the study “shows that there is whole layer of biology that we haven’t even anticipated”.
The brain is watching
After sensing an intruder, the immune system unleashes a flood of immune cells and compounds that promote inflammation. This inflammatory response must be controlled with exquisite precision: if it’s too weak, the body is at greater risk of becoming infected; if it’s too strong, it can damage the body’s own tissues and organs.
Previous work has shown that the vagus nerve, a large network of nerve fibres that links the body with the brain, influences immune responses. However, the specific brain neurons that are activated by immune stimuli remained elusive, says Hao Jin, a neuroimmunologist at the US National Institute of Allergy and Infectious Diseases in Bethesda, Maryland, who led the work.
To investigate how the brain controls the body’s immune response, Jin and his colleagues monitored the activity of brain cells after injecting the abdomen of mice with bacterial compounds that trigger inflammation.
How the brain senses a flu infection — and orders the body to rest
The researchers identified neurons in the brainstem that switched on in response to the immune triggers. Activating these neurons with a drug reduced the levels of inflammatory molecules in the mice’s blood. Silencing the neurons led to an uncontrolled immune response, with the number of inflammatory molecules increasing by 300% compared with the levels observed in mice with functional brainstem neurons. These nerve cells act as “a rheostat in the brain that ensures that an inflammatory response is maintained within the appropriate levels”, says study co-author Charles Zuker, a neuroscientist at Columbia University in New York City.
Further experiments revealed two discrete groups of neurons in the vagus nerve: one that responds to pro-inflammatory immune molecules and another that responds to anti-inflammatory molecules. These neurons relay their signals to the brain, allowing it to monitor the immune response as it unfolds. In mice with conditions characterized by an excessive immune response, artificially activating the vagal neurons that carry anti-inflammatory signals diminished inflammation.
Dampening autoimmune symptoms
Finding ways to control this newly discovered body–brain network would offer an approach to fixing broken immune responses in various conditions such as autoimmune diseases and even long COVID, a debilitating syndrome that can persist for years after a SARS-CoV-2 infection, Jin says.
Cracking the genetic code of autoimmune disease
There’s evidence that therapies targeting the vagus nerve can treat diseases such as multiple sclerosis and rheumatoid arthritis, suggesting that targeting the specific vagal neurons that carry immune signals might work in people, Zuker says. But, he cautions, “it’s a lot of work to go from here to there”.
Besides the neuronal network identified in the study, there might be other routes through which the body transmits immune signals to the brain, says Stephen Liberles, a neuroscientist at Harvard Medical School in Boston, Massachusetts. What’s more, the mechanisms by which the brain sends signals back to the immune system to regulate inflammation remain unclear. “We’re just scratching the surface,” he says. “We need to understand the rule book of how the brain and the immune system interact.”
Every year, between 250,000 and 300,000 people in Germany suffer from a stroke or heart attack. These patients suffer immune disturbances and are very frequently susceptible to life-threatening bacterial infections. Until now, little was known about the underlying mechanisms of this immune dysfunction. Research teams from the Faculty of Medicine at the University Hospital of the UDE and the Leibniz Institute for Analytical Sciences in Dortmund have now uncovered a previously unknown cause – and a therapeutic approach. These findings are published in the May 2024 issue of the Journal Nature Cardiovascular Research.
The study was led by Prof. Matthias Gunzer, Director of the Institute of Experimental Immunology and Imaging (IEIB) at the UDE and Head of the Biospectroscopy Department at the Leibniz Institute for Analytical Sciences (ISAS), and Dr. Vikramjeet Singh, Head of the Stroke Immunology Unit at the IEIB. They found that in patients one to three days after a stroke or heart attack, the amount of IgA antibodies in the blood decreases drastically – these are essential for defense against infections. Antibodies come in several subtypes, collectively known as immunoglobulins (Ig), which are produced by specialized plasma cells.
To track down the mechanism behind the loss of antibodies – and to improve the treatment of patients with these findings – the researchers used disease mouse models. Mice also experienced a loss of IgA in their blood and stool after a stroke or heart attack. The researchers discovered that specialized DNA fibers released in blood are a factor in the loss of immune defense. These DNA fibers, known as neutrophil extracellular traps (NETs), originate from the nuclei of another type of immune cell, neutrophils. NETs are released into the blood in large quantities by highly activated neutrophils after a stroke or heart attack and can directly kill plasma cells in the intestine. Probably an even more important effect of NETs is the formation of hundreds of small clots in the blood vessels that supply energy to plasma cells in the intestine. This results in a lack of nutrient and oxygen supply and the Ig-forming cells die off in large numbers.
The immunologists and their teams not only succeeded in proving a causal link between stroke, heart attack and immunodeficiency, but they were also able to demonstrate a new treatment approach: If the NETs were destroyed with the enzyme DNase or their release was prevented by a substance with a novel mode of action, the immune defense remained intact. The researchers were able to demonstrate this both in the mouse model and – in the case of DNase – in later clinical studies.
Until now, no therapeutic approaches could be developed because the cause of the immune deficiency was unclear. A treatment that breaks down the NETs or even prevents them from forming in the first place could be a promising new approach to maintaining the immune defense in patients after a stroke or heart attack. It may be possible to prevent serious secondary infectious diseases or even death.”
Prof. Matthias Gunzer, Director of the Institute of Experimental Immunology and Imaging (IEIB) at the UDE and Head of the Biospectroscopy Department at the Leibniz Institute for Analytical Sciences (ISAS)
Tuz, A. A., et al. (2024). Stroke and myocardial infarction induce neutrophil extracellular trap release disrupting lymphoid organ structure and immunoglobulin secretion. Nature Cardiovascular Research. doi.org/10.1038/s44161-024-00462-8.
Liver inflammation, a common side-effect of cancers elsewhere in the body, has long been associated with worse cancer outcomes and more recently associated with poor response to immunotherapy. Now, a team led by researchers from the Abramson Cancer Center and Perelman School of Medicine at the University of Pennsylvania has found a big reason why.
In their study, published today in Nature Immunology, the researchers discovered that cancer-induced liver inflammation causes liver cells to secrete proteins called serum amyloid A (SAA) proteins, which circulate through the body and hinder the ability of T cells-;major anticancer weapons of the immune system-;to infiltrate and attack tumors elsewhere.
We want to better understand what causes cancer to resist or respond to immunotherapy to help design more effective strategies for patients. Our findings show that liver cells-;with their release of SAA proteins-;effectively serve as an immune checkpoint regulating anti-cancer immunity, making them a promising therapeutic target.”
Gregory Beatty, MD, PhD, senior author, associate professor of Hematology-Oncology and the director of Clinical and Translational Research for the Penn Pancreatic Cancer Research Center
The study builds on previous research from the team, including co-lead authors Meredith Stone, PhD, a research associate, and Jesse Lee, a graduate student, into liver inflammation in cancer: In a 2019 study, they showed how it promotes pancreatic tumor metastasis to that organ. In 2021, researchers from the Beatty Laboratory observed that systemic inflammation, involving many of the same molecules implicated in liver metastasis, is associated with worse responses to immunotherapies in pancreatic cancer patients. The latest study was designed to investigate in more detail how liver inflammation may block the effects of these immune-boosting therapies.
First, they looked at mouse models of pancreatic cancer, measuring the amount of T-cell infiltration in pancreatic tumors-;a basic indicator of anti-tumor immune activity. They found that mice with less T cell infiltration in their tumors tended to have more liver inflammation. These mice also showed stronger signs of an inflammatory signaling pathway called the IL-6/JAK/STAT3 pathway-;the same one the team had implicated in liver metastasis in their 2019 study.
The researchers next showed that STAT3 activation in liver cells is associated with the reduced production of immune cells called dendritic cells, which are critical for normal T cell responses. When the scientists deleted STAT3 from liver cells, dendritic cell production and T cell activity picked up, and tumors that previously had only low T cell-infiltration developed high T cell-infiltration.
Ultimately the team found that STAT3 activation in liver cells has its dendritic cell- and T cell-suppressing effect by inducing the production of SAA proteins, which target receptors on immune cells. Deleting the SAA proteins had the same immune-restoring effect as deleting STAT3, and increased survival times and the likelihood of cures in mice that had pancreatic tumors surgically removed.
To get a sense whether the mouse model findings would translate to humans, the researchers measured SAA levels in tissue samples from patients whose pancreatic tumors had been surgically removed and found that those with low SAA levels at surgery went on to have significantly longer survival times afterward.
“The translational findings in human patients highlight the likely clinical relevance of our discoveries in the mice,” Beatty said. “Now that we’ve shown how liver inflammation puts up a roadblock to immunotherapy, our next step is to see if the same pathway can be targeted to reverse inflammation in patients who already have liver metastasis.”
The research team is now working to set up further preclinical and eventually clinical studies of STAT3- and/or SAA-inhibiting agents as potential add-on therapies in combination with immunotherapy-;for example, prior to surgery-;that could improve cancer patient outcomes.
Support for the research was provided by the National Institutes of Health (T32 CA009140, T32-HL007439-41, K12-CA076931-21, R01-CA197916, R01CA245323, U01 CA224193 and U01 CA224175), the Damon Runyon Cancer Research Foundation, the PacMen Consortium, the US Department of Defense (W81XWH2110622, W81XWH2110621), Stand Up to Cancer, the Robert L. Fine Cancer Research Foundation, the Penn-Wistar SPORE in Skin Cancer, AACR-The Mark Foundation for Cancer Research, and the Pancreatic Cancer Action Network.
Stone, M. L., et al. (2024). Hepatocytes coordinate immune evasion in cancer via release of serum amyloid A proteins. Nature Immunology. doi.org/10.1038/s41590-024-01820-1.
Macrophages are evolutionarily conserved phagocytes ubiquitously present in almost all organs and tissues. It is recognized that the umbrella term macrophage comprises highly heterogeneous cells with diverse functions and roles.
RTMs are stable, long-lived subpopulations in different organs and tissues and have been linked to innate immunity and the pathogenesis of chronic inflammatory diseases. However, RTMs have broader functions beyond immunity.
Recently, exploring RTM subsets to functional, developmental, and spatial levels has become feasible, helping identify mechanisms of tissue homeostasis.
Notwithstanding these advances, substantial knowledge gaps remain. In the present review, researchers provided insights into conditions impacting RTM identity, division of labor among RTM subsets, and RTM dysfunction in disease.
Tissue microenvironment impacts RTM development
RTMs originate from embryonic progenitors or hematopoietic stem cell (HSC)-derived monocytes. The local microenvironment influences the trajectories of RTM differentiation upon seeding a tissue. In homeostasis, the local environmental cues shape RTM cell identity in a tissue-specific manner.
Further, the phenotypic and functional convergence of HSC-derived monocytes towards a tissue-specific RTM program is driven by the local environment.
However, inflammation or disease markedly impacts their differentiation. During such disturbance, the differentiation of HSC-derived monocytes skews toward pro-reparative, tumor-supportive, or pro-inflammatory phenotypes, differing from that of steady-state RTMs.
These inflammation-associated macrophages (iMacs) are short-lived, and upon resolution (of the disturbance), the tissue transitions to a distinct state, i.e., inflammation aftermath.
There may be permanent changes in the original homeostatic distribution and the composition of environmental factors. This was demonstrated in white adipose tissue, where HSC-derived RTMs acquired a more inflammatory phenotype following the resolution of chronic inflammation.
This post-inflammation scar led to HSC-derived RTMs being unable to differentiate into their original cellular state.
Coexistence of RTM subsets within tissues
Historically, it has been believed that organs and tissues are populated by unique tissue-specific RTMs during homeostasis, such as Langerhans cells in the skin, alveolar macrophages (AMs) in the lungs, Kupffer cells in the liver, and microglia in the brain.
However, a seminal work from 2010 showed that embryonic yolk sac progenitors, not monocytes, give rise to microglia.
This was also instrumental in revealing the embryonic origin of other RTMs. Studies have demonstrated that two distinct conserved RTM subsets populate most tissues in the interstitial space.
The authors term these RTM subsets as perivascular macrophages (PVMs). The PVMs precede with the name of the organ/tissue of residence.
Of the conserved PVM subsets, T cell immunoglobulin and mucin domain containing 4 (TIM4+) PVMs emerge during embryogenesis in multiple organs and are characterized by low levels of major histocompatibility complex II (MHCII) and high levels of TIM4, folate receptor beta (FOLR2), lymphatic vessel endothelial hyaluronan receptor 1 (LYVE1), and cluster of differentiation 206 (CD206).
By contrast, MHCII+ PVMs emerge from HSC-derived monocytes and are characterized by low/intermediate levels of FOLR2 and LYVE1 and high levels of CD206 and MHCII.
While some studies have observed a C-C motif chemokine receptor 2 (CCR2+) PVM subset, they are likely to be recent organ immigrants. Although some organs have unique tissue-specific subsets of RTMs, almost all organs share these two conserved PVMs.
Division of labor among RTMs
Microglia are the only brain RTM subset in contact with neurons. Several fundamental microglial functions beyond immunity have been uncovered more recently. Animal studies have shown that microglia are essential in neuronal development and fitness.
Microglia secrete growth factors critical for synapse formation. Additionally, they survey the brain microenvironment and modulate neuronal activity through synaptic engulfment and pruning.
Recent studies have revealed the presence of PVMs in perivascular spaces of the central nervous system (CNS). Further, these PVMs regulate cerebrospinal fluid (CSF) dynamics, and TIM4+ PVMs in the brain facilitate proper extracellular matrix (ECM) dynamics.
This idea was corroborated by the findings of abnormal ECM deposition and deterioration of CSF flow dynamics in aged mice, which are linked to a smaller ratio of brain TIM4+-to-MHCII+ PVMs.
The distinct locations of lung PVMs indicate they have specialized roles. For instance, lung MHCII+ PVMs may regulate neuronal interaction with stromal cells, whereas lung TIM4+ PVMs contribute to lung homeostasis.
Besides, lung TIM4+ PVMs may be involved in wound healing, while the MHCII+ counterparts may be involved in antigen presentation and immune activation.
Heart MHCII+ and TIM4+ PVMs produce growth factors to support proper cellular functions and adjust to physiologic demands. Cardiac PVMs are in close contact with cardiomyocytes and participate in mutual electric conduction, supporting normal cardiac contractions.
Gut muscularis MHCII+ and TIM4+ PVMs are close to blood vessels, myenteric plexus, and submucosal plexus. Gut MHCII+ PVMs are closely associated with neuronal bodies of the enteric nervous system.
Mechanistically, gut muscularis PVMs secrete bone morphogenetic protein 2 (BMP2) to regulate enteric neurons expressing the BMP2 receptor. Besides, they regulate gastrointestinal motility independent of the enteric nervous system. Recent studies suggest that gut PVMs promote neuroprotection and limit neuronal cell death.
RTM dysregulation and disease
It is established that HSC-derived iMacs are linked to chronic inflammatory diseases. This chronicity is thought to be due to ongoing inflammation leading to tissue function loss.
Nevertheless, how dysfunction or deviation of RTMs’ core homeostatic functions cause disease remains less studied. Usually, deviation is required for proper tissue repair.
However, it is not clear how long-term and persistent deviation affects tissue physiology and disease severity. Pulmonary alveolar proteinosis is caused by AM dysfunction, characterized by protein and surfactant accumulation in the lung alveolar space, limiting proper gas exchange and increasing susceptibility to infections.
This can occur due to mutations in the granulocyte-macrophage colony-stimulating factor (GM-CSF), autoantibodies against GM-CSF, or silica inhalation. Further, the absence or dysfunction of lung TIM4+ PVMs can result in increased fibrosis and loss of tissue function.
Likewise, dysregulation of heart TIM4+ PVMs exacerbates fibrosis following cardiac infarction. Loss of RTM’s core homeostatic functions may impact cancer development.
A recent study on breast cancer patients showed that those harboring tumors with increased breast TIM4+ PVMs had improved survival rates and T cell priming against the tumor.
This suggested that enhancing the TIM4+ PVMs’ homeostatic functions while inhibiting the activity of HSC-derived tumor-related macrophages can be effective for treatment.
Further, disruption of ECM remodeling in brain PVMs is associated with aging and Alzheimer’s disease (AD).
Concluding remarks
Taken together, ontogeny and local environmental cues shape the phenotype and heterogeneity of RTMs.
There is a strong division of labor among RTM subpopulations. The study proposed a unifying nomenclature for the two conserved RTM subpopulations and explored the roles of several unique tissue-specific RTM subsets in homeostasis and disease.
Nevertheless, further studies are required to delineate how RTM dysfunction leads to chronic inflammatory diseases fully.
Aging is a primary risk factor for chronic illnesses, marked by reduced physiological capabilities. Cell senescence, genomic instability, stem cell fatigue, and mitochondrial failure are characteristics.
Aging also increases the risk of chronic illnesses such as Alzheimer’s disease, atherosclerosis, osteoarthritis, type 2 diabetes, chronic obstructive pulmonary disease (COPD), and cancer. Healthy habits like calorie control and regular physical exercise help prevent age-related disorders.
However, small-molecule therapies have limits, and vaccines provide a potential technique to target specific antigens to generate immune responses.
About the review
In the present review, researchers present new developments in vaccines using senescent cells to target the etiological agents of aging and related diseases.
Immunology of senolytic vaccines that target aging
Vaccines stimulate the innate immunological system, making it rapidly respond to infection. This reaction activates adaptive immune cells, causing humoral antibodies to manufacture antibodies and cell-mediated immunity to attack infected cells. Vaccinations lead to pathogen-targeted memory cell development to accelerate response to reinfections. Vaccines targeting microbes, cell populations, or chemicals can prevent and treat disease development. Senolytic vaccines, which target senescent cells, have been demonstrated to reduce arterial plaque development.
These vaccination techniques provide new pathways for managing age-associated disorders, with advantages such as fewer injections, increased patient adherence, cost-effectiveness, and improved targeting efficiency.
Senolytic vaccinations target senescent cells by targeting chemicals on their surfaces, using peptide-based platforms to eradicate them through complement-dependent cytotoxicity (CDC) or natural killer (NK) cell-mediated and antibody-dependent cell-mediated cytotoxicity (ADCC).
Membrane proteins overexpressed in senescent cells are used as vaccine antigens or immune cell targets to stimulate the development of specific antibodies.
Tumor-associated antigens (TAAs) and tumor-specific antigens (TSAs) trigger a cluster of differentiation 4-expressing helper T cells, CD8+ cytotoxic T cells, and B cells to kill cancer cells.
Cancer vaccines use cell-based, virus-based, peptide-based, and nucleic acid-based platforms to stimulate adaptive immunity.
Research on vaccine-based strategies for age-related disorders
Alzheimer’s disease (AD) vaccinations attempt to lower the brain’s amyloid-beta (Aβ) and tau protein levels by stimulating the adaptive immune system to produce antibodies. Peptides with neuroprotective properties are potentially possible therapies.
Vaccines like ACI-24, UB-311, AV-1959D, ABvac40, ACI-35, AADvac1, and GV1001 target Aβ and tau proteins in innate immune cells. ACI-24 targets Aβ1-15 liposomes, UB-311 targets Aβ protein, AV-1959D targets deoxyribonucleic acid (DNA), ABvac40 targets Aβ protein, ACI-35 targets tau protein accumulation, and AADvac1 and GV1001 demonstrate long-term safety, tolerance, and immunogenicity.
Type 2 diabetes vaccinations target molecules like dipeptidyl-peptidase 4 (DPP4) and interleukin-1 beta (IL-1β) to restore levels and prevent problems.
The vaccines use peptide sequences to produce anti-DPP4 antibodies, increase glucose tolerance, restore beta cell mass, and reduce IL-1β production. They also couple prorenin epitopes with keyhole limpet hemocyanin (KLH), improving retinal blood circulation, decreasing microglia activation, and reducing gliosis and vascular leakage in diabetic rats.
Vaccines for age-related vascular diseases such as hypertension, abdominal aortic aneurysm (AAA), and atherosclerosis target molecules that regulate blood pressure, cholesterol, and blood vessel function. PMD-2850, PMD-3117, CYT006-AngQb, AT1R, ATRQβ-001, and ADR-004 inhibit angiopoietin 1 (Ang I) and age-related accumulation in hypertensive rats.
Vaccines containing KLH and Ang II decreased macrophage aggregation in the AAA wall, suppressed tumor necrosis factor (TNF) expression, and protected against elastic fiber injury.
The nerve growth factor (NGF) protein is an osteoarthritis target. Researchers covalently linked recombinant NGF proteins to virus-like particles (VLPs) derived from a cucumber mosaic virus with tetanus toxoid epitopes.
Vaccinated mice developed measurable antibodies against NGF and showed reversed pain behavior. ADAM metallopeptidase domain 12 (ADAM12) and GLI family zinc finger 1 (GLI1) levels are associated with fibrosis. Lentiviral vectors that encode these proteins decrease fibrotic activity in mice.
Proprotein convertase subtilisin/kexin type 9 (PCSK9) can treat fibrosis. PCSK9Qβ-003, an epitope peptide, enhanced kidney fibrosis, and increased fatty acid beta-oxidation-associated variables among Ldlr+/− murine animals. The vaccine can treat kidney fibrosis, hypercholesterolemia, and atherosclerosis.
Conclusions
Based on the review findings, senescent cells play a significant role in age-related chronic disorders and demonstrate immunogenicity, making them candidates for targeted vaccine elimination.
However, vaccinations can cause adverse effects such as injection site redness, discomfort, fever, and headaches. Continuous evaluation of vaccination safety is required to comprehend long-term adverse effects.
Vaccines targeting key mediators in age-related disorders have seldom proven efficacy in slowing disease development. Researchers must select antigens from key disease drivers or investigate epitopes generating robust immune responses to boost vaccination effectiveness.
Combinatorial therapy incorporating vaccinations and immunomodulatory medications may be more effective.