mRNA vaccines developed against the spike glycoprotein of severe acute respiratory syndrome type 2 coronavirus (SARS-CoV-2), displayed remarkable efficiency in combating coronavirus 19 (COVID-19). These vaccines work by triggering both cellular and humoral immune responses against the spike protein of the virus. Cellular immunity may play a more protective role than humoral immunity to variants of concerns (VOC) against SARS-CoV-2, as it targets the conserved regions of spike protein and possibly cross-reacts with other variants.
Since a single spike epitope is recognized by multiple T-cell clones, the mRNA vaccination-induced T-cell response may consist of multiple spike-reactive clones. Thus, it is important to understand the mechanism of mRNA vaccination-induced cellular immune response. However, to address this clonal-resolution analysis on T-cell responses to mRNA vaccination has not been performed yet.
To bridge this gap, a team of researchers, led by Associate Professor Satoshi Ueha, including Professor Kouji Matsushima from the Tokyo University of Science (TUS), Japan, Mr. Hiroyasu Aoki from the University of Tokyo, and Professor Toshihiro Ito from Nara Medical University, aimed to develop a kinetic profile of spike-reactive T-cell clones during repetitive mRNA vaccination. For this, they performed a longitudinal TCR sequencing on peripheral T cells of 38 participants who had received the Pfizer vaccine from before the vaccine to after the third vaccination and then analyzed the single-cell gene expression and epitope specificity of the clonotypes.
Their findings, published in Cell Reports on March 7, 2024, revealed that while the primary T-cell response of naïve T cells generally peaked 10-18 days after the first shot, expansion of “early responders” was detected on day 7 after the first shot, suggesting that these early responders contain memory T cells against common cold coronaviruses. They also found a “main responder” that expanded after the second shot and did not expand early after the first shot and a “third responder” that appeared and expanded only after the third shot.
By longitudinally tracking the total frequency of each response pattern, it was observed that, after the second shot, a shift among the clonotypes occurred, wherein the major population changed from early responders to main responders, suggestive of a shift in clonal dominance. A similar shift of responding clones was also observed in CD4+ T cells.
We next analyzed the phenotype of main responders after the second and the third vaccination. The results showed that the main responders after the second and third shots mostly consist of effector-memory T cells (TEM), with more terminally differentiated effector memory-like phenotype after the third shot.”
Satoshi Ueha, Associate Professor, Tokyo University of Science
The researchers then examined the repertoire changes of main responders, revealing that the expansion of main responders, which occurred after the second shot, diminished following the third shot, and the clonal diversity decreased and was partially replaced by the third responders. This may potentially mean that the third vaccination selected better-responding clones.
Due to the vaccination-induced shift in immunodominance of spike epitopes, the study supports the inter-epitope shift model. In addition, there were intra-epitope shifts of vaccine-responding clonotypes within spike epitopes.
Prof. Ueha explains the significance of these results, “Our analysis suggests that T cells can “re-write” themselves and reshape their memory populations after successive vaccinations. This re-writability not only maintains the number of memory T cells but also maintains diversity that can respond to different variants of pathogens. Moreover, by tuning the replacement of memory cells, more effective vaccines can be developed that can also be tailored to an individual’s unique immune response.”
Overall, this study provides important insights into mRNA vaccine-induced T-cell responses, which will be crucial for developing next-generation vaccines for more effective and broad protection against viruses.
Aoki, H., et al. (2024) CD8+ T cell memory induced by successive SARS-CoV-2 mRNA vaccinations is characterized by shifts in clonal dominance. Cell Reports. doi.org/10.1016/j.celrep.2024.113887.
A team of University of Michigan researchers has successfully modified a naturally occurring chemical compound in the lab, resulting in advanced lead compounds with anti-HIV activity.
Their results, published March 7 in the Journal of Medicinal Chemistry, offer a new path forward in the development of drugs that could potentially help cure-;rather than treat-;HIV.
Although effective treatments are available to manage HIV, a cure has remained elusive due to the virus’s ability to hide from the immune system, lying dormant in reservoirs of infected cells.
With most viruses, when people get infected, they get sick for a while and then the immune system kicks in and the virus is cleared. But with HIV, once a patient is infected, that virus will persist for their entire life-;meaning they must remain on treatments indefinitely.”
Kathleen Collins, Professor, Microbiology and Immunology, University of Michigan
One key to HIV’s ability to remain hidden in patients’ cells is a protein that the virus makes, called Nef. This protein shuts down a system that the cell would normally use to alert the immune system to an infection, thus preventing the immune cells from recognizing and clearing the virus.
Collins and her lab have studied this protein for more than 15 years, investigating how it works and how it can be disabled. She and David Sherman, professor at the U-M Life Sciences Institute, previously discovered that a chemical found in nature can inhibit HIV Nef, allowing the immune system to find and eliminate virally infected cells: a compound called concanamycin A (CMA), which is produced by a soil-derived microorganism.
In its natural form, however, CMA presents several challenges as a potential therapeutic. The first challenge the team had to overcome was supply. While CMA is a naturally occurring compound, the original bacteria that produces it does so in quantities far too small to be useful for testing and modification in the lab.
Another major challenge with developing CMA as an anti-HIV drug is that Nef is not CMA’s primary target.
“CMA’s main job in human cells is to inhibit an enzyme called V-ATPase, which we absolutely do not want to block in this case,” said Sherman, who is also a professor at the U-M College of Pharmacy, Medical School, and College of Literature, Science, and the Arts. “So, we needed to find a way to modify CMA’s activity, widening the effective dosage gap between when it starts to inhibit the target we’re aiming for-;HIV Nef -; without affecting V-ATPase, its typical cellular target.”
With this latest research, the team has overcome both of these challenges. Using bioengineering, Sherman’s team was able to develop a bacterial strain that increased CMA production 2,000-fold. Synthetic chemists in the lab then created more than 70 new variations of the compound, swapping out different chemical groups, to test for their potency against HIV Nef.
Collins’ lab team ran the new compounds through a battery of tests to measure their toxicity to cells, as well as how they affected the activities of both HIV Nef and V-ATPase.
“Even though we know that CMA is extremely active against the HIV Nef protein, all drugs have side effects,” said Collins, also a professor of internal medicine at the Medical School. “And so we wanted to ensure we’ve done everything we can to minimize the side effect profile of the drug before we consider putting it into an animal or human.”
The team now has several CMA analogs that show high potency in blocking HIV Nef at very low dosage levels, without interrupting off-target effects or causing toxicity in human cells. They caution, however, that several important steps remain before the compounds would be ready for further testing in a clinical setting.
“We are really encouraged, though, because our groups have solved some very important problems,” Sherman said. “We have engineered microorganisms to produce sustainable supplies of the natural product molecules and have really good chemical methods to make new analogs. And we have the methodologies in place to continue tracking the critical toxicity and potency parameters to further reduce off-target effects.”
Source:
Journal reference:
McCauley, M., et al. (2024). Structure–Activity Relationships of Natural and Semisynthetic Plecomacrolides Suggest Distinct Pathways for HIV-1 Immune Evasion and Vacuolar ATPase-Dependent Lysosomal Acidification. Journal of Medicinal Chemistry. doi.org/10.1021/acs.jmedchem.3c01574.
Insights into the workings of an immune cell surface receptor, called PD-1, reveal how treatments that restrict its action can potentially be strengthened to improve their anticancer effect, a new study shows. The same findings also support experimental treatment strategies for autoimmune diseases, in which the immune system attacks the body, because stimulating the action of PD-1, as opposed to restricting it, can potentially block an overactive immune response.
Led by researchers at NYU Langone Health’s Perlmutter Cancer Center and the University of Oxford, the study is publishing in the journal Science Immunology online March 8.
The study results revolve around the body’s immune system, which is primed to attack virally infected and cancerous cells while leaving normal cells alone. To spare normal cells from immune attack, the system uses “checkpoints,” sensors on the surface of immune cells, including T cells, which turn them off or dampen activation when they receive the right signal. The immune system recognizes tumors as abnormal, but cancer cells can hijack checkpoints to turn off immune responses.
Among the most important checkpoints is a protein called programmed cell death receptor 1 (PD-1), which is shut down by a relatively new drug class called checkpoint inhibitors to make tumors “visible” again to immune attack. Such drugs are at least somewhat effective in a third of patients with a variety of cancers, say the study authors, but the field is urgently seeking ways to improve their performance and scope.
At the same time, PD-1 signaling is slowed in autoimmune diseases like rheumatoid arthritis, lupus, and type 1 diabetes, such that the action of unchecked immune cells creates inflammation that can damage tissues. Agonists, drugs that stimulate PD-1, are now showing promise in clinical trials.
Many immune checkpoints are receptors on the surface of T cells that act to translate docking information from the outside of the cell to the signaling portion of the receptor inside the cell. Connecting the outside-of-the-cell portion of PD-1 with the inside portion is the transmembrane segment. Many immune receptors function in pairs called dimers, but to date, PD-1 has been thought to function alone, not in the dimer form.
Study results showed that PD-1 forms a dimer through interactions of its transmembrane segment. Researchers say this finding is in sharp contrast to other immune receptors, which typically form dimers through the segment of the receptor that is outside the cell.
Further immune cell testing in mice showed that encouraging PD-1 to form dimers, specifically in the transmembrane domain but not in its outer or inner regions, increased its ability to suppress T cell activity, while decreasing transmembrane dimerization lowered PD-1’s ability to inhibit immune cell activity.
Our study reveals that the PD-1 receptor functions optimally as dimers driven by interactions within the transmembrane domain on the surface of T cells, contrary to the dogma that PD-1 is a monomer.”
Elliot Philips, MD, PhD, Study Lead Investigator and Physician-Scientist, NYU Grossman School of Medicine
Elliot Philips is an internal medicine resident at NYU Grossman School of Medicine and Perlmutter Cancer Center. Philips is also an alumnus of the Vilcek Institute of Biomedical Sciences at NYU.
“Our findings offer new insights into the molecular workings of the PD-1 immune cell protein that have proven pivotal to the development of the current generation of anticancer immunotherapies, and which are proving essential in the design and developing of the next generation of immunotherapies for autoimmune diseases,” said study co-senior investigator and cancer immunologist Jun Wang, PhD. Wang is an assistant professor in the Department of Pathology at NYU Grossman and Perlmutter.
“Our goal is to use our new knowledge of the functioning of PD-1 to determine if weakening its dimerization, or pairing, helps make anticancer immunotherapies more effective, and just as importantly, to see if strengthening its dimerization helps in the design of agonist drugs that quiet overactive T cells, tamping down the inflammation seen in autoimmune diseases,” said study co-senior investigator and structural biologist Xiang-Peng Kong, PhD. “Presently, research efforts have focused on strengthening PD-1 interactions with its ligands, or signaling molecules, involved with inhibiting T cell action.
“Our new study suggests that efforts to design better drugs should focus on increasing or decreasing PD-1’s dimerization to manipulate T cell function,” said Kong, a professor in the Department of Biochemistry and Molecular Pharmacology at NYU Grossman and Perlmutter.
Among the study’s other findings was that a single change in the amino acid structure of the transmembrane segment can act to either enhance or diminish the inhibitory function of PD-1 in immune responses. The team plans further investigations of PD-1 inhibitors and agonists to see if they can tailor what they say are more effective, “rationally designed” therapies for both cancer and autoimmune disorders.
Funding support for the new study was provided by National Institutes of Health grants R01AI125640, R37CA273333 T32AR069515, and T32GM007308. Additional funding support was provided by NYU Grossman School of Medicine, Kennedy Trust for Rheumatology Research grant 100262Z/12/Z; Research Council of Norway grant 275466, in conjunction with Marie Sklodowska-Curie Actions; Wellcome Trust grant 108869/Z/15/Z; the Melanoma Research Alliance; and a pilot award from the NYU Colton Center for autoimmunity. Wang has been a paid consultant to RootPath Genomics, Bristol Myers Squibb, and Hanmi Pharmaceutical and is a founder, equity holder, and consultant to Remunix. These interests and relationships are being managed in accordance with the policies of NYU Langone Health.
Besides Philips, Wang, and Kong, other NYU Langone researchers involved in this study are colead investigator Jia Liu, and coinvestigators Charles Ng, Ian Ahearn, Ruimin Pan, Christina Luo, Alexander Leithner, Zhihua Qin, and Dan Littman, who is also a Howard Hughes Medical Institute investigator. Other study coinvestigators include Audun Kvalvaag, at Oslo University, Norway; Alexander Morch and co-senior investigator Michael Dustin, at the University of Oxford, United Kingdom; Anna Tocheva, at the Icahn School of Medicine at Mount Sinai in New York; Hong Liang and Yong Zhou, at the University of Texas in Houston; Antonio Garcia-Espana, at the University of Rovira i Virgili in Tarragona, Spain; and Adam Mor, at Columbia University in New York.
Source:
Journal reference:
Philips, E. A., et al. (2024) Transmembrane domain–driven PD-1 dimers mediate T cell inhibition. Science Immunology. doi.org/10.1126/sciimmunol.ade6256.
Nature, Published online: 06 March 2024; doi:10.1038/d41586-024-00426-9
Direct interactions between cells in tissue are incompletely understood because the advanced technologies required to examine them are still in their infancy. A new method can decipher cell–cell interactions on a large scale.
T follicular helper cells (Tfh) are essential for strong antibody-mediated reactions of our immune system during infections and vaccinations. However, if they get out of control, this can cause diseases such as autoimmunity, allergies or cancer. Researchers from the University Hospital Bonn (UKB) and the Cluster of Excellence ImmunoSensation at the University of Bonn investigated the underlying mechanisms of Tfh cell development in a mouse model and thus decoded their internal networking. They hope that this will lead to new strategies for the development of highly effective vaccines and new therapies to combat various diseases. The results have now been published in the renowned journal Science Immunology.
T follicular helper cells (Tfh cells) are a specialized subgroup within the so-called CD4+ T helper cells in the immune system. Their main task is to assist the B cells in the immune defense. They are essential for the generation of highly effective antibodies. Tfh cells therefore play a decisive role in protecting against and fighting infections. “Although Tfh cells were first described over 20 years ago, there is still no reliable protocol for their generation in cell culture,” says co-first author Dr. Yinshui Chang, former postdoctoral researcher at the University of Bonn at the UKB, describing the motivation to take a closer look at the process in the mouse model.
The transforming growth factor TGF-β is a cytokine. This is a group of proteins that initiates and regulates the growth and differentiation of cells. The Bonn team led by Prof. Dr. Dirk Baumjohann has now discovered that this signaling molecule induces strong protein expression of both the transcription factor Bcl6 and the chemokine receptor CXCR5, which are characteristic of Tfh cells. The latter plays an important role in the targeted migration of Tfh cells into the vicinity of B cells.
We were able to show that the Tfh cells induced by TGF-β in cell culture are quite similar to the Tfh cells generated in a living organism. They provide crucial help for B cells.”
Luisa Bach, co-first author, doctoral student at the University of Bonn at the UKB
Transcription factor c-Maf controls the fate of T helper cells
Using a new method based on CRISPR gene scissors, the international team led by the Bonn researchers discovered that the production of CXCR5 induced by TGF-β is independent of the transcription factor Bcl6, but requires the transcription factor c-Maf. Remarkably, although Tfh and Th17 cells partially undergo common developmental stages, c-Maf acts as a switching factor for Tfh versus Th17 cell fates. Th17 cells are another special type of CD4+ T helper cells and play an important role in bacterial infections and autoimmune diseases.
“Overall, our data clarify important aspects of the long-unclear prerequisites and molecular pathways for the development of Tfh cells. They also highlight the diverse functions of the transforming growth factor TGF-β. Furthermore, these data indicate that Tfh cell development in mice and humans may not be as different as we previously assumed,” says Prof. Baumjohann from the Medical Clinic III for Hematology, Oncology, Immuno-Oncology and Rheumatology at the UKB, who is a member of the Cluster of Excellence ImmunoSensation and the Transdisciplinary Research Area (TRA) “Life & Health” at the University of Bonn. “Importantly, our findings may have implications for the development of new therapeutic strategies that enhance Tfh cells during vaccinations and infections or inhibit them in autoimmune and allergic diseases.”
Chang, Y., et al. (2024) TGF‑β specifies TFH versus TH17 cell fates of murine CD4+ T cells through c-Maf. Science Immunology. doi.org/10.1126/sciimmunol.add4818.
A perplexing problem for people with recurring urinary tract infections (UTIs) is persistent pain, even after antibiotics have successfully cleared the bacteria.
Now Duke Health researchers have identified the likely cause – an overgrowth of nerve cells in the bladder.
The finding, appearing March 1 in the journal Science Immunology, provides a potential new approach to managing symptoms of recurring UTIs that would more effectively target the problem and reduce unnecessary antibiotic usage.
“Urinary tract infections account for almost 25% of infections in women,” said senior author Soman Abraham, Ph.D., professor in the departments of Pathology, Molecular Genetics and Microbiology, Integrative Immunobiology, and Cell Biology at Duke University School of Medicine.
“Many are recurrent UTIs, with patients frequently complaining of chronic pelvic pain and urinary frequency, even after a round of antibiotics,” Abraham said. “Our study, for the first time, describes an underlying cause and identifies a potential new treatment strategy.”
Abraham and colleagues collected bladder biopsies from recurrent UTI patients who were experiencing pain despite no culturable bacteria in their urine. Using biopsies from people without UTIs as a comparison, they found evidence that sensory nerves were highly activated in the UTI patients, explaining the persistent sense of pain and urinary frequency.
Further studies in mice revealed the underlying events, with unique conditions in the bladder that prompt activated nerves in the lining to bloom and grow with each infection.
“Typically, during every bout of UTI, epithelial cells laden with bacteria are sloughed off, and significant destruction of nearby nerve tissue occurs,” said Byron Hayes, lead author of the study and previously a postdoctoral fellow in Duke’s Department of Pathology. “These events trigger a rapid repair program in the damaged bladder involving massive regrowth of destroyed nerve cells.”
This immune response, including repair activities, is led by mast cells – which are immune cells that fight infection and allergens. Mast cells release chemicals called nerve growth factor, which drive overgrowth and increase sensitivity of nerves. The result is pain and urgency.
The researchers were able to address these symptoms by treating study mice with molecules that suppress production of the mast-cell generated nerve growth factor.
This work helps illuminate a puzzling clinical condition that drives medical costs and affects the quality of life of millions of people, primarily women,” Abraham said. “Understanding the crosstalk between mast cells and nerves is an essential step toward effective treatments for people suffering repeat urinary tract infections.”
Soman Abraham, Ph.D., Senior Author
In addition to Abraham and Hayes, study authors include Hae Woong Choi, Abhay PS Rathore,Chunjing Bao, Jianling Shi, Yul Huh, Michael W Kim, Andrea Mencarelli, Pradeep Bist, Lai Guan Ng, Changming Shi, Joo Hwan Nho, Aram Kim, Hana Yoon, Donghoon Lim, Johanna L Hannan, J Todd Purves, Francis M Hughes Jr, and Ru-Rong Ji.
The study received funding support from the National Institutes of Health (K12-DK100024, R01-DK121969, R01-DK121032, R01-GM144606), the National Research Foundation of Korea (2020R1C1C1003257), and a Korea University grant.
There lies a paradox in sleep. Its apparent tranquility juxtaposes with the brain’s bustling activity. The night is still, but the brain is far from dormant. During sleep, brain cells produce bursts of electrical pulses that cumulate into rhythmic waves – a sign of heightened brain cell function.
But why is the brain active when we are resting?
Slow brain waves are associated with restful, refreshing sleep. And now, scientists at Washington University School of Medicine in St. Louis have found that brain waves help flush waste out of the brain during sleep. Individual nerve cells coordinate to produce rhythmic waves that propel fluid through dense brain tissue, washing the tissue in the process.
These neurons are miniature pumps. Synchronized neural activity powers fluid flow and removal of debris from the brain. If we can build on this process, there is the possibility of delaying or even preventing neurological diseases, including Alzheimer’s and Parkinson’s disease, in which excess waste – such as metabolic waste and junk proteins – accumulate in the brain and lead to neurodegeneration.”
Li-Feng Jiang-Xie, PhD, first author, postdoctoral research associate in the Department of Pathology & Immunology
The findings are published Feb. 28 in Nature.
Brain cells orchestrate thoughts, feelings and body movements, and form dynamic networks essential for memory formation and problem-solving. But to perform such energy-demanding tasks, brain cells require fuel. Their consumption of nutrients from the diet creates metabolic waste in the process.
“It is critical that the brain disposes of metabolic waste that can build up and contribute to neurodegenerative diseases,” said Jonathan Kipnis, PhD, the Alan A. and Edith L. Wolff Distinguished Professor of Pathology & Immunology and a BJC Investigator. Kipnis is the senior author on the paper. “We knew that sleep is a time when the brain initiates a cleaning process to flush out waste and toxins it accumulates during wakefulness. But we didn’t know how that happens. These findings might be able to point us toward strategies and potential therapies to speed up the removal of damaging waste and to remove it before it can lead to dire consequences.”
But cleaning the dense brain is no simple task. Cerebrospinal fluid surrounding the brain enters and weaves through intricate cellular webs, collecting toxic waste as it travels. Upon exiting the brain, contaminated fluid must pass through a barrier before spilling into the lymphatic vessels in the dura mater – the outer tissue layer enveloping the brain underneath the skull. But what powers the movement of fluid into, through and out of the brain?
Studying the brains of sleeping mice, the researchers found that neurons drive cleaning efforts by firing electrical signals in a coordinated fashion to generate rhythmic waves in the brain, Jiang-Xie explained. They determined that such waves propel the fluid movement.
The research team silenced specific brain regions so that neurons in those regions didn’t create rhythmic waves. Without these waves, fresh cerebrospinal fluid could not flow through the silenced brain regions and trapped waste couldn’t leave the brain tissue.
“One of the reasons that we sleep is to cleanse the brain,” Kipnis said. “And if we can enhance this cleansing process, perhaps it’s possible to sleep less and remain healthy. Not everyone has the benefit of eight hours of sleep each night, and loss of sleep has an impact on health. Other studies have shown that mice that are genetically wired to sleep less have healthy brains. Could it be because they clean waste from their brains more efficiently? Could we help people living with insomnia by enhancing their brain’s cleaning abilities so they can get by on less sleep?”
Brain wave patterns change throughout sleep cycles. Of note, taller brain waves with larger amplitude move fluid with more force. The researchers are now interested in understanding why neurons fire waves with varying rhythmicity during sleep and which regions of the brain are most vulnerable to waste accumulation.
“We think the brain-cleaning process is similar to washing dishes,” neurobiologist Jiang-Xie explained. “You start, for example, with a large, slow, rhythmic wiping motion to clean soluble wastes splattered across the plate. Then you decrease the range of the motion and increase the speed of these movements to remove particularly sticky food waste on the plate. Despite the varying amplitude and rhythm of your hand movements, the overarching objective remains consistent: to remove different types of waste from dishes. Maybe the brain adjusts its cleaning method depending on the type and amount of waste.”
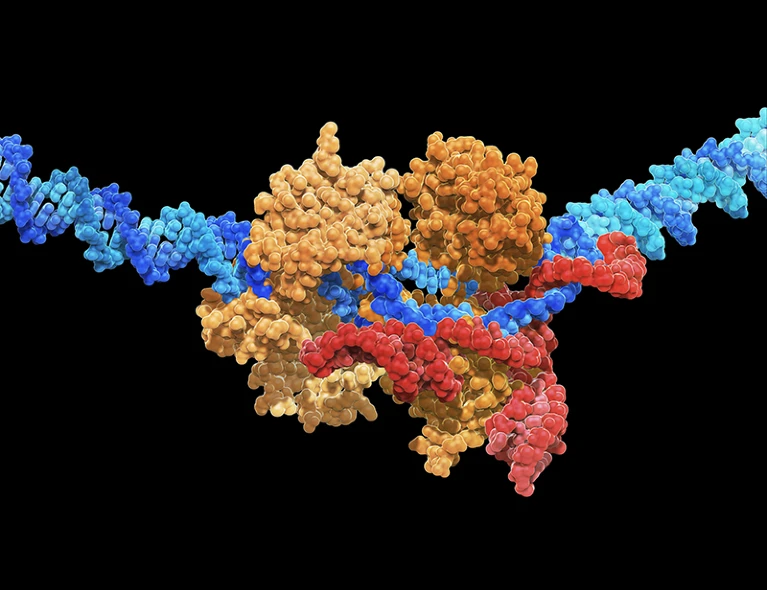
Gene-editing systems, such as CRISPR-Cas9, can be used to give stem cells immune-evasive properties.
CARLOS CLARIVAN/SPL
After decades of development, the dream of regenerative medicine has become a clinical reality — in part. Researchers can now cultivate stem cells in a laboratory, transform them into specialized cell types and then transplant them into people to alleviate disease.
In theory, this strategy promises an endless supply of replacement parts for ailing and ageing bodies: neurons to combat Parkinson’s disease, insulin-producing pancreatic cells to reverse type 1 diabetes, heart muscle cells to enhance cardiac function, and more.
But there’s a catch: therapies derived from stem cells must be customized to the patient — a process that is both slow and expensive. Or they can be made using donor cells. But, because the immune system tends to reject foreign cells, these ‘allogeneic’ off-the-shelf treatments require the concurrent administration of immune-dampening medicines — a strategy that raises the risk of complications such as infection and cancer.
Innovations in Gene Therapy
Now, researchers are exploring a third approach — one that could fully realize the vision of mass-produced cell therapies for everyone, without the need for immune suppression.
By harnessing the power of gene-editing techniques, particularly CRISPR–Cas systems, to endow stem cells with immune-evasive properties, researchers can fashion stem cells that circumvent the immune system’s recognition mechanisms. They can also incorporate fail-safe features to ensure that the cells can be eliminated in the event of unforeseen complications. Such ‘stealth’ cells could, in principle, underpin a wide range of cell-replacement therapies, and billions of dollars have been invested in this work over the past five years.
The idea still requires validation. Only a small number of people have so far received any form of cell-replacement therapy derived from immune-edited stem cells, and no clinical results have yet been publicly disclosed. But with more products of this kind slated to enter human testing later this year, researchers are optimistic.
“We know in theory that it will work,” says Torsten Meissner, an immunologist at Beth Israel Deaconess Medical Center in Boston, Massachusetts, who points to the natural precedent of immune evasion to underscore his conviction: “Tumours have figured it out. Viruses have figured it out. Pregnancy is the other example.” Now, he says, biotechnology companies just need to work out how to emulate the same tactics for therapeutic gain.
Incognito mode
Strategies differ, but there are some gene edits that all researchers agree must underpin any universal stem-cell-derived therapy. There is also widespread consensus that the optimal product should incorporate as few edits as possible, both to minimize the potential for unintended genetic consequences and to streamline manufacturing and regulatory approval.
Beyond that, the scientific community is divided. The complexities of the immune system have fuelled spirited debates over the exact genetic manipulations necessary to create a cell therapy that is both capable of bypassing immune defences and delivering meaningful health benefits.
“The immune system is pervasive and persistent,” says Charles Murry, a cardiovascular pathologist at the University of Washington in Seattle and chief executive of StemCardia in Seattle, one of a growing number of biotechnology companies developing gene-editing strategies to overcome immune barriers in regenerative cell treatments.
It might take the immune system a while to find donor cells, Murry notes, “but find them it does. It’s ancient, smart and has lots of tricks up its sleeves.” Researchers must, therefore, be equally crafty when designing cells to evade it.
Could CAR-T-cell therapy offer hope to children with cancer?
In most cases, the process starts by disrupting at least one part of the cell’s major histocompatibility complex (MHC), a cluster of proteins that functions like a molecular identity card, displaying unique pieces of cellular information that tell the immune system’s foot soldiers — a group of cells known as T lymphocytes — whether the cell is friend or foe.
“That’s the ‘universal’ element of the universal donor cell,” Murry explains. This edit strips the transplanted cell of its enemy identity, allowing it to seamlessly blend into its new environment and evade T-cell detection.
But the lack of MHC expression also presents a problem. Without the usual distinguishing markers of either ally or adversary, the edited cell becomes susceptible to attack by a different set of immune actors — natural killer (NK) cells, which have evolved to target and eliminate abnormal cells, including those without the proper MHC signatures.
To counteract this vulnerability, some researchers reintroduce genes that encode specific MHC antigens — ones that allow the cell to temper NK cells without inciting T-cell responses. Others are putting in genes that express ‘checkpoint’ proteins, molecules designed to directly curb the activity of NK cells.
Sana Biotechnology in Seattle, which favours the latter approach, reported last year that just three edits — two to eliminate MHC expression and one to boost expression of a checkpoint protein called CD47 — were sufficient to shield cells of rhesus monkeys (
Macaca mulatta ) from the animals’ immune systems
1
. It also showed that human cells, modified in the same manner, could ameliorate diabetes when transplanted into a mouse model
2
.
In November, Sana announced that it had the go-ahead to begin testing, in people, of donated human pancreatic cells that had been edited in this way. Trials of a stem-cell-derived product are likely to follow.
But not everyone has managed to replicate the findings around CD47. And with conflicting reports about how best to restrain NK-cell activity, stem-cell biologist Audrey Parent at the University of California, San Francisco (UCSF), sees that piece of the immune-evasion puzzle as the primary bottleneck in the field. “The NK cell part is not resolved yet,” she says.
Covert agents
Disagreement around NK-cell inhibition arises, at least in part, from the various methods laboratories use to assess the modified cells’ ability to evade immune detection. Although most research groups evaluate their edited stem cells in engineered mice with human-like immune systems, these ‘humanized’ models cannot faithfully replicate the complete immune response that cell products will face in people’s bodies.
Pancreatic cells could potentially be edited to treat diabetes.
Credit: LENNART NILSSON, BOEHRINGER INGELHEIM INTERNATIONAL GmbH/SPL
Conversely, others generate gene-edited stem cells from monkeys and transplant them into other monkeys, mirroring the clinical scenario with humans. But this strategy is constrained by ethical concerns and the expense of experimentation with primates. Moreover, monkeys, although genetically similar to people, have distinct immune systems that might not faithfully reflect human responses.
Deepta Bhattacharya, an immunologist at the University of Arizona in Tucson, favours a different approach. When it comes to pushing the boundaries of immune evasion, he advocates evaluating universal gene-edited products that are intended for human use in mice with fully intact, natural immune systems. If cell therapies can pass this cross-species test, he reasons, they should be well-suited for transplantation into any human recipient.
Early this year, Bhattacharya and his colleagues reported that human stem cells containing a battery of 12 gene edits could survive in mice for months, with no signs of immune recognition or rejection
3
.
“A few of [the edits] we don’t think we actually need,” Bhattacharya says. But some edits that he considers crucial for thwarting rejection target a branch of the body’s natural defence mechanism known as the complement system. This system acts as a first line of defence against potential invaders by preparing antibodies to mark and eliminate foreign cells.
“Antibodies are tricky,” says Chad Cowan, co-founder and chief executive of Clade Therapeutics, a Boston-based biotech firm that is developing stem-cell-derived therapies for cancer and autoimmune conditions. (Bhattacharya is also a scientific co-founder.) “I think we’ve solved the cellular side of the equation,” Cowan says. “But antibodies actually turn out to be a bigger barrier than we thought.”
Clade’s solution, currently unpublished, involves engineering cells to secrete an enzyme that degrades and incapacitates nearby antibodies, thereby neutralizing the complement system. Another approach comes from Sonja Schrepfer, head of the hypoimmune platform at Sana who, together with UCSF heart surgeon Tobias Deuse and their colleagues, reported last year that overexpression of a protein that binds and disables antibodies can achieve the same result
4
.
Neither approach has been vetted in people — and, as molecular endocrinologist Timothy Kieffer at the University of British Columbia in Vancouver points out: “Strategies to thwart the highly evolved immune system are numerous, but are only hypothetical until proven otherwise.”
“The true test can only come in clinical trials,” he says.
Kieffer is also chief scientific officer of Fractyl Health, a metabolic therapeutics company in Lexington, Massachusetts. But two years ago, while serving as chief scientific officer for ViaCyte in San Diego, California, Kieffer played a pivotal part in launching the first clinical study of a stem-cell-derived product that incorporated immune-cloaking edits.
This pioneering product, developed in collaboration with biotech firm CRISPR Therapeutics in Boston, was named VCTX210. Designed to help people with type 1 diabetes to produce their own insulin, the product incorporated a suite of four gene edits collectively intended to enhance immune evasion and bolster cell survival. A subsequent version of this therapy, termed VCTX211, included an additional two edits, each aimed at further enhancing the robustness and functionality of the cells.
Invisibility shield
How effective these therapies were at sidestepping immune detection and improving the control of type 1 diabetes remains unclear. As
Nature went to press, no results had been publicly disclosed. And both Vertex (which acquired ViaCyte in 2022, but is now working on separate stem-cell-derived therapies, using gene-editing technologies from CRISPR Therapeutics) and CRISPR Therapeutics (which now wholly owns the VCTX210 and VCTX211 assets) declined to comment on their immune-evasive cell-therapy programmes.
Also unclear is whether any safety concerns emerged in these trials. This matter is of utmost importance to researchers such as Kieffer because, as he explains, “concerns arise with manipulating the genome of cells for therapy, particularly when the goal is to endow them with an invisibility cloak that could be problematic should the cells become dangerous to the recipient”.
In the ViaCyte-CRISPR-Therapeutics trials, the companies took the precautionary step of
encapsulating
their immune-evasive cells in small, sticking-plaster-sized pouches, which are then implanted beneath the person’s skin. These devices contain pores that allow blood vessels to enter, providing oxygen and nutrients to the metabolically active cells inside, but prevent any therapeutic cells from escaping. If any unanticipated issues arise, they can be swiftly retrieved before rogue cells cause widespread damage.
Turbocharged CAR-T cells melt tumours in mice — using a trick from cancer cells
Another safety measure involves the integration of genetic fail-safe features into the edited cells themselves. These features include drug-inducible suicide genes that can be activated by administration of a relatively benign medication. Researchers are also adorning modified cells with surface proteins that can be targeted with clinically approved antibody drugs, thereby achieving the same goal of cell destruction should any transplants turn cancerous or problematic in other ways.
In the end, the optimal safety strategy — not to mention the ideal amount of gene editing necessary to tamp down immune responses — can vary with the disease. A ready-to-use cell therapy for cancer does not necessarily need to incorporate the same design features as one tailored for diabetes, for instance, given the differences in the immune system that these cell products will confront and the distinct risk–benefit consideration in each disease. “There is no one catch-all solution,” Meissner says.
Certain parts of the body, including the eye and the brain, also enjoy an ‘immune privileged’ status, meaning that only a limited set of immune cells can enter them. This has led companies such as BlueRock Therapeutics in Cambridge, Massachusetts, which is developing off-the-shelf stem-cell-derived therapies for Parkinson’s disease, to tailor their immune-editing strategies accordingly. “There are some unique opportunities when you’re in the brain,” says BlueRock’s head of immunology, Greg Motz.
Those opportunities won’t be the last word on universal cell therapies, of course. Rather, Murry expects to see incremental advancement in the field, with short-term wins and losses informing long-term editing strategies.
“I would love it to be perfect out of the gates, but that’s not realistic,” Murry says. “This is going to be like peeling an onion.”
As Canada’s flu season collides with record strep A cases and ongoing COVID-19 concerns, a new study is shedding light on our understanding of respiratory immune responses. Scholars from the Research Institute of the McGill University Health Centre (RI-MUHC) have discovered a surprising facet about a century-old vaccine for tuberculosis, Bacillus Calmette Guérin (BCG). The study, published in the journal Nature Immunology, uncovered a previously unknown mechanism that extends the vaccine’s shield to combat influenza A virus-;the most prevalent flu strain.
The immune interactions involved here can ‘train’ the lungs, which are frequently exposed to infectious agents in the environment. If we can map out the protective immune pathways involved in the lungs, this will revolutionize our conceptual and clinical approaches in developing vaccines against infections, including emergent respiratory viruses.”
Maziar Divangahi, lead author, pulmonary immunologist, senior scientist at the RI-MUHC, and Professor of Medicine at McGill University
The discovery paves the way for future studies to assess whether BCG could be used to prevent other emergent viruses. Notably, research on the vaccine’s protection against COVID-19 has had promising results.
Source:
Journal reference:
Tran, K. A., et al. (2024). BCG immunization induces CX3CR1hi effector memory T cells to provide cross-protection via IFN-γ-mediated trained immunity. Nature Immunology. doi.org/10.1038/s41590-023-01739-z.
Omalizumab was given to children who were severely allergic to peanuts and at least two other foods.Credit: Patrick Sison/AP via Alamy
For people with food allergies, accidentally eating the wrong thing could prove deadly. Now, for the first time, an asthma drug has been shown to protect people from severe reactions if they ingest a small amount of a food they’re allergic to.
In a study reported on 25 February in the New England Journal of Medicine1, researchers tested a drug called omalizumab in 3 adults and 177 children aged between one and 17 who were severely allergic to peanuts and at least two other foods. After about four months of treatment, 67% of those who received the drug were able to ingest the equivalent of two or three peanuts without it causing a significant reaction, compared with just 7% of those who received a placebo. Omalizumab seemed to be similarly effective at raising participants’ tolerance to other foods they were allergic to, including cashews, milk and eggs.
Research round-up: Allergies
“This is a huge breakthrough for food-allergy treatment,” says Ruchi Gupta, a paediatrician at Northwestern University Feinberg School of Medicine in Chicago, Illinois. She points out that although the drug doesn’t offer an outright cure for food allergies, it lowers the risk that ingesting a trace amount of the food will prove catastrophic. “Having treatments that can make people feel safer [while eating] is just wonderful.”
On the basis of this evidence, the US Food and Drug Administration (FDA) approved omalizumab as a treatment for food allergies earlier this month.
Nature looks at the promise and limitations of the new treatment, and other ways food allergies could be treated in the future.
How does omalizumab work?
Omalizumab, known commercially as Xolair, isn’t a new drug: the FDA approved it for the treatment of asthma in 2003 and, later, for chronic hives and for nasal polyps that occur with certain breathing conditions.
The drug is a monoclonal antibody designed to attack a specific type of human antibody known as IgE. Like other antibodies, IgE is produced by immune cells when the body perceives a specific protein to be a threat. But if that protein is an allergen, such as peanut protein or cat dander, IgE causes unnecessary inflammation that can prompt the body to go into anaphylactic shock. Omalizumab recognizes all kinds of IgE antibody — including those that attack air pollutants in asthma and those that attack food proteins. Researchers have long suspected that the drug could also be useful for treating food allergies, Gupta says.
The drug must be injected once every two to four weeks, depending on the allergic person’s weight and the severity of their reaction, and can cost more than US$1,400 per injection.
What makes it different from other treatments?
The FDA has approved only one other treatment for a food allergy — a peanut-protein powder called Palforzia. Approved in 2020 for children aged four years and over, Palforzia works by allowing the immune system to build up a tolerance to peanuts over time. This is done by gradually increasing the dosage over the course of about six months. Conversely, omalizumab starts to work immediately and has been shown to be safe in children as young as one year old.
Moreover, because the monoclonal antibody attacks all kinds of IgE antibody, it can be used for allergies to foods other than peanuts. “It theoretically should work as well for any different food allergy that that person has,” says the study’s lead author Robert Wood, a paediatric allergy specialist at Johns Hopkins University School of Medicine in Baltimore, Maryland. He says omalizumab might also work for other autoimmune conditions that people taking it have, such as pollen allergies and eczema.
What are the drug’s limitations?
The study didn’t find any adverse side effects associated with taking omalizumab. But Wood cautions that lowering a person’s natural IgE antibody defences could make them more vulnerable to infection with parasitic worms.
Perhaps the drug’s most important limitation is that it doesn’t eliminate allergies — it only raises the threshold for the amount of food a person can eat before it triggers a reaction. In the FDA’s statement approving omalizumab, the agency said that people taking the drug “must continue to avoid foods they are allergic to”.
“The biggest worry is that patients may be assuming that their protection from food reactions is pretty complete,” Wood says. He says researchers will be monitoring whether people who take the drug start taking more risks and having more reactions as a result.
What don’t we know about it?
Although omalizumab increases the amount of food needed to trigger an allergic reaction, Gupta says it’s not clear whether it can decrease the severity of a reaction if a person goes far over that limit — consuming a handful of peanuts, for example.
And Wood says he and others are now studying why the results varied so widely between individuals: at the end of the trial, 14% of the participants who took omalizumab were still unable to consume even a fraction of one peanut without having a reaction. Working out why some people don’t respond well, he says, will help clinicians to determine who will benefit most from the drug.
What other food-allergy treatments are on the horizon?
Researchers are currently testing another monoclonal antibody approved for the treatment of asthma and eczema, dupilumab, in people with peanut allergies. Dupilumab targets signalling molecules, released by immune cells, that trigger inflammation. And researchers are testing a eczema drug called abrocitinib, which blocks certain types of signalling pathway in immune cells, as a treatment for multiple food allergies.
Other trials are testing simpler treatments. Gupta, for instance, is studying whether feeding four-month-old infants small amounts of eight common allergens such as wheat and shellfish can head off the development of allergies. “Having new choices for treatments is really just going to help this field so much,” she says.