Root of Tripterygium wilfordii Celastrol is produced in the root of the traditional medicinal plant Tripterygium wilfordii. Credit: Nikolaj Hansen
A traditional Chinese medicinal plant has huge potential as a weight loss drug. However, due to the plant’s notorious toxicity, no one has yet succeeded in exploiting it effectively. Researchers from the University of Copenhagen have not only found the formula for the synthetic production of the compound – they have even found a simple and sustainable recipe using ordinary yeast as the main ingredient.
In China, children are taught to steer clear of this plant. The plant, Thunder god vine (Chinese: 雷公藤), which in China has earned the nickname “Seven Steps to Death,” is so poisonous that a person risks death only a few steps after consuming it.
But despite its deadliness, the Thunder god vine (Tripterygium wilfordii) hides something quite beneficial to us humans as well. Within its roots, the plant produces the compound celastrol, a chemical agent with powerful anti-obesity properties.
Experiments using mice on a high fat diet have shown that the mice given celastrol gained 45% less weight than the control group. Experiments with human cells have shown similar effects.
HOW THE DRUG WORKS
Some people are able to eat a lot without gaining weight because our metabolism knows when we eat a lot and secretes certain hormones that cause us to burn more calories. One of these hormones is leptin.
People who are overweight become resistant to leptin due to an overproduction of the hormone, which leads to an inflammation of the hypothalamus. As a result, the body does not receive the signal. Celastrol re-sensitizes the body to leptin.
The effect is due to the fact that celastrol reactivates the body’s sensitivity to leptin, a hormone to which overweight people become resistant. Leptin is one of the hormones that causes the body to burn more calories and thereby regulate weight.
How does one get their hands on the ‘good’ substance without the toxicity that typically accompanies it? That is the question.
“For obvious reasons, a person cannot just eat the plant and benefit from the drug. So what do we do? The problem with extracting celastrol from the nature source is that it is very hard to separate it from the other toxic molecules that the plant is full of. So far, there has been no effective method to achieve this,” says Sotirios Kampranis, professor at the Department of Plant and Environmental Sciences.
Yong Zhao and Sotirios Kampranis Yong Zhao and Sotirios Kampranis with celastrol produced in yeast cells Credit: Yao-Tao Duan
Yeast as ‘surrogate mother’
In approaching the problem, the research team from the Department of Plant and Environmental Sciences sought to find a way to produce the substance biotechnologically. Led by Assistant Professor Yong Zhao, the researchers were the first to map the pathway with all 15 biochemical steps that the plant undergoes as it forms celastrol. These steps are vital to know in order to recreate the substance biosynthetically.
THUNDER GOD VINE
The plant, Thunder god vine, which in Latin is called Tripterygium wilfordii, has been used for thousands of years in traditional Chinese medicine to treat rheumatoid arthritis and as a contraceptive.
The plant grows in the mountainous regions of Southern China, where local collectors harvest it. Thus, in addition to being extremely toxic, it is also difficult to find.
“The compound is extracted from the plant root. And the plant takes at least three years to grow large enough for it to be harvested. Therefore, an entire plant must be sacrificed to acquire the drug. So it is not a tenable way,” Sotirios Kampranis points out.
“We found out how the plant forms celastrol by finding all of the steps in the manufacturing process. This means that we could take the genes and enzymes that make the substance and put them into another organism that does not produce toxic substances. And that’s what we’ve done with yeast,” says Yong Zhao.
The researchers were able to produce synthetic celastrol in a tank with ordinary yeast that was used as a host organism within which the substance was produced.
“Imagine, you just need to feed the celastrol molecule table sugar, and by doing so, you get a compound that is almost in pure form without the toxic compounds that otherwise come with it in nature. The process is simple and effective – it only takes around a week to get the final product. And it takes place without the toxic solvents or catalysts that are typically used in chemical syntheses. I believe there is a huge potential here,” says Sotirios Kampranis.
Isolated celastrol Isolated celastrol produced by the Kampranis lab. Celastrol is a complex plant specialized metabolite with a reddish color. Credit: Yong Zhao
The greenest – and only – method
Today, most pharmaceuticals are created through synthesis based on crude oil-based petrochemicals. And the traditional ways of developing synthetic drugs are actually not even an option, as Yong Zhao explains:
“Because the celastrol molecule is so complex, there are currently only very inefficient chemical synthesis methods which are not applicable for large-scale production. So our method is not only a green method – it is also the only real method that exists.”
The researchers point out that yeast is widely used in the biotech industry, where one finds all the necessary know-how and infrastructure to produce celastrol at a large scale.
“That is precisely why we have chosen to use yeast as an organism. While academics develop the technology, it is important that it comes in a form that is useful for industry, where the technology can be further developed to make products that can help us all,” says Sotirios Kampranis.
The next step is more closely investigating the drug’s potential to treat obesity in humans. The researchers hypothesize that a potential treatment can either be done with celastrol alone or combined with other therapies.
“For example, one can imagine a treatment where celastrol is combined with other anti-obesity drugs to achieve a more robust effect. Because the more targets in the body that are hit, the better. Indeed, one often sees a synergistic effect when several agents are at play simultaneously. But here, of course, the pharmaceutical industry must take over,” says Yong Zhao.
Reference: “Biosynthesis and biotechnological production of the anti-obesity agent celastrol” by Yong Zhao, Nikolaj L. Hansen, Yao-Tao Duan, Meera Prasad, Mohammed S. Motawia, Birger L. Møller, Irini Pateraki, Dan Staerk, Søren Bak, Karel Miettinen and Sotirios C. Kampranis, 26 June 2023, Nature Chemistry. DOI: 10.1038/s41557-023-01245-7
The researchers behind the study are: Yong Zhao, Nikolaj L. Hansen, Yao-Tao Duan, Meera Prasad, Mohammed S. Motawia, Birger L. Møller, Irini Pateraki, Dan Staerk, Søren Bak, Karel Miettinen and Sotirios C. Kampranis, all from the Department of Plant and Environmental Sciences and the Department of Drug Design and Pharmacology at the University of Copenhagen.
The University of Copenhagen has filed for a patent application for the invention and is currently in talks with potential partners about commercializing the method.
The project is supported by the Novo Nordisk Foundation.
In a recent review published in the International Journal of Obesity, researchers explored the potential of glucagon-like peptide-1 (GLP-1) analog treatments to change food preferences and consumption and reduce obesity.
They concluded that while results show that GLP-1 lowers appetite and consumption in the short term, they rely on self-reports of intake. Further studies are needed to assess weight maintenance using objective intake measurements.
Of the three primary interventions for obesity, namely surgical intervention, lifestyle changes, and medication, pharmacology has emerged as minimally invasive, promisingly effective at reducing weight, and more sustainable in the long term.
GLP-1 analog medications such as semaglutide and liraglutide are often prescribed to manage obesity. Recent studies have focused on the mechanisms underlying their effect on weight loss, specifically how they alter food preferences and consumption.
About the study
This review focused on GLP-1 analog drugs, assessing how they have been studied and synthesizing what is currently known about their effects. Authors located relevant research through the medical literature database PubMed using search terms such as ‘obesity,’ ‘semaglutide,’ ‘liraglutide,’ and ‘GLP-1 analog.’
Results were filtered to ensure that they pertained to studies with human and rodent participants and had been published within a timeframe of 25 years. Outcomes were restricted to taste preference, food consumption, weight loss, and maintenance. Information related to publication year, location, methods, results, and study type were noted.
Findings
Researchers have studied ingestion behaviors through food and drink monitors and commonly rely on verbal reports and visual analog scales to assess fullness and satiety. Self-reported data are used to assess food preferences and eating control.
Studies using functional magnetic resonance imaging (fMRI) have found that people who use GLP-1 analog drugs show lowered responses to pictures of food, particularly in brain regions associated with reward and appetite, such as the amygdala, insula, orbitofrontal cortex, and putamen.
Semaglutide appears to target circumventricular organs instead of breaching the blood-brain barrier, binding with GLP-1 receptors, and modifying food preferences by interacting with amphetamine- and cocaine-regulated transcripts and proopiomelanocortin neurons.
After semaglutide treatment, individuals lose weight for 12-18 months before their weight stabilizes during the maintenance phase. People taking semaglutide said they felt less desire for salty, spicy, high-fat, sweet, and savory foods, craved less starch and dairy, and faced less difficulty resisting cravings and controlling their food intake. However, animal studies suggest semaglutide treatment could also increase low- and mid-range sucrose consumption.
During the weight reduction phase, patients consumed smaller meals and showed lower preferences for energy-rich food, leading to less energy consumption. Studies have not reported ingestive behavior during the maintenance phase, so whether patients return to their original food habits is unknown.
Some gastrointestinal effects of semaglutide, such as diarrhea, constipation, nausea, and vomiting, have been reported, but beginning at lower medication doses has been found to address this issue.
Another GLP-1 analog drug, liraglutide, reduces hunger and increases feelings of satiation during the initial phase by binding with GLP-1 receptors in the arcuate nucleus and subcortical brain region, stimulating proopiomelanocortin neurons. It may slow gastric emptying, but how it could do so has not been established.
Conclusions
The evidence suggests that GLP-1 analog drugs alter food preferences and reduce food cravings and intake, which could lead to long-term weight loss and maintenance. However, animal studies also indicate that these drugs could increase sucrose consumption, which should be examined in humans.
Less attention has been paid to ingestive, appetitive, and consummatory behavior in the weight maintenance phase. Instead, most studies have focused on the weight loss phase, and many have asked participants to report on their own cravings, portion control, and appetite.
While such data is easier to collect, it may lead to biases related to recall and social desirability, and objective measurements are needed to understand the effects of anti-obesity drugs.
The authors note that the weight-loss effects of GLP-1 analogs are now well-established and that new medications are under development.
Understanding the behavioral mechanisms through which these drugs take effect using human and rodent studies can allow researchers and health practitioners to refine treatments and tailor interventions to the needs of individual patients, enhancing overall outcomes.
Further, focusing on the weight maintenance phase of treatment can reduce unrealistic expectations by patients and their clinicians and lead to less propagation of misinformation regarding the drugs’ long-term effects, which could threaten the willingness of people to use these medications to treat obesity in the future.
Journal reference:
Changes in food preferences and ingestive behaviors after glucagon-like peptide-1 analog treatment: techniques and opportunities. Bettadapura, S., Dowling, K., Jablon, K., Al-Humadi, A.W., le Roux, C.W. International Journal of Obesity (2024). DOI: 10.1038/s41366-024-01500-y, https://www.nature.com/articles/s41366-024-01500-y
Depression is a chronic mood disorder that is associated with low mood, insomnia, weight loss, a state of unhappiness, aversion to activity, fatigue, and low self-esteem. According to the World Health Organization, depression has become one of the major health burdens across the world.
This mental health condition is commonly treated with an antidepressant that takes around a month to alleviate the symptoms. However, several side effects are associated with the use of antidepressant drugs and could be toxic at high doses.
A combination of psychological, genetic, and neurological factors contributes to the manifestations of depression. Even though the exact etiology of this mental health issue is not fully understood, research has shown chronic stress to be an inducer of depression.
The hippocampus is a region of the brain that is associated with depression and modifies functionally and morphologically in response to stress. Animal model studies have shown that a decrease in neuronal and glial size, reduction in synaptic markers, loss of dendrites, and increase in apoptosis in the hippocampus leads to depression.
Many studies have uncovered the metabolic aspects of depression. For instance, diabetes and obesity are two common metabolic disorders that increase the risk of depression. Considering its high prevalence, novel therapies with high efficacy and fewer side effects are required to combat depression. The chronic mild stress (CMS) model has been recognized as a reliable rodent model to study depression.
Glucagon-like peptide-1 (GLP-1) and its receptor agonists are involved with anti-inflammatory effects and neuroprotective activities and can improve mental disorders, particularly depression and cognition. GLP-1 is a peptide hormone that stimulates the secretion of insulin and restricts the synthesis of glucagon in the pancreas in a glucose-dependent manner. Liraglutide is a GLP-1 analog that exhibited a positive effect in reducing anxiety and depression symptoms.
Dulaglutide is a novel long-acting GLP-1 receptor agonist that improves cognitive dysfunction and neuronal damage in rats with vascular dementia. Although many studies highlighted the efficacy of dulaglutide in preventing depression-like behavior triggered by chronic social defeat stress (CSDS), the underlying mechanism of this effect is not clearly understood.
About the study
The current study used a metabolomics strategy to evaluate the effect of dulaglutide in a CMS model. Furthermore, the underlying mechanism of this effect was also assessed. Adult male ICR mice, which is a strain of albino mice, were selected for this study. All test mice were around seven weeks old.
After one week of acclimatization, 60 mice were randomly assigned in four groups, namely, control (CON), the CMS and Vehicle group (CMS+Veh), the CMS and 0.3 mg/kg dulaglutide group (Low Dula), and the CMS and 0.6 mg/kg dulaglutide group (High Dula). Except for the CON group, all other groups were exposed to stressors.
To establish the CMS model of depression, selected mice were exposed to two or three different stressors for 28 days continuously. For stress induction, mice were deprived of water and food for 12 hours, kept in wet bedding for 24 hours, kept in a tilted cage for 24 hours, pintail for 1 minute, and cold water treatment for five minutes. The body weight of each test mouse was measured weekly, and behavioral tests, such as the tail suspension test (TST), open field test (OFT), and forced swimming test (FST), were performed.
Study findings
The mice subjected to CMS for four weeks exhibited depressive- and anxiety-like symptoms. An LC-MS/MS metabolomics study was performed to understand the potential pathophysiological mechanisms and investigate the efficacy of drugs to alleviate depression-like symptoms.
A distinct difference between the CON group, CMS+Veh group, and High Dula group was observed in accordance with the metabolic disorders induced by chronic stress, which was altered through dulaglutide treatment. Many potential biomarkers were identified that are associated with purine metabolism, arginine and proline metabolism, glycerophospholipid metabolism, glutamate metabolism, sphingolipid metabolism, and bile secretion.
Lipid metabolism pathways could be potential targets through which dulaglutide alleviates depression. Lysophosphatidylcholine (LPC), phosphatidylethanolamine (PE), lysophosphatidylethanolamine (LPE), phosphatidylinositol (PI), sphingolipids, and phosphatidylcholine (PC), are involved with the therapeutic effect of dulaglutide in alleviating depression. Consistent with previous studies findings, this study highlighted the association between lipid metabolism and the antidepressant effect of dulaglutide.
The current study indicated the downregulation of N-acetyl-L-aspartic acid (NAA) in the CMS model group. NAA, which is one of the most important metabolites of the vertebrate nervous system, was found in decreased levels in rats with chronic, unpredictable, mild stress. However, the current study indicated that dulaglutide therapy increased the levels of NAA through its upregulation in the hippocampus.
In the CMS model group, an upregulation in L-glutamic acid and L-arginine was observed. Dulaglutide treatment caused a decrease in arginine and proline, thereby indirectly exhibiting a neuroprotective effect.
Conclusions
The current study highlighted the antidepressant effects of dulaglutide using the CMS depression model. Notably, the potential metabolisms that underlie the antidepressant effect of dulaglutide have been elucidated in this study.
For women undergoing autologous breast reconstruction – reconstruction using the patient’s own tissues, rather than implants – the risks of overall and specific complications are increased at higher body mass index (BMI) levels, reports the March issue of Plastic and Reconstructive Surgery®, the official medical journal of the American Society of Plastic Surgeons (ASPS). The journal is published in the Lippincott portfolio by Wolters Kluwer.
Our study clarifies the impact of high BMI as a risk factor for adverse outcomes of autologous breast reconstruction. It also suggests that, among patients with obesity, losing weight before surgery might lower the risk of complications.”
Merisa Piper, MD, senior author of University of California, San Francisco
How does BMI affect autologous breast reconstruction outcomes?
Autologous breast reconstruction, typically using a flap of tissue from the abdomen, is an alternative for reconstruction after mastectomy for breast cancer. Autologous reconstruction offers advantages including stable breast reconstruction with fewer surgical procedures, in less time, and at lower cost, compared to implant-based reconstruction.
However, not all patients are optimal candidates for this procedure: risk factors for adverse outcomes include smoking, uncontrolled diabetes, and high BMI. Despite previous studies, the impact of high BMI on outcomes of autologous breast reconstruction remain unclear.
Dr. Piper and colleagues analyzed the impact of BMI on outcomes of autologous reconstruction in 365 patients (545 breasts) between 2004 and 2021. All patients underwent microvascular breast reconstruction using an abdominal-based flap. Complications were assessed for patients in different BMI categories, ranging from normal weight (less than 25 kg/m2), to overweight (25 to 29.9 kg/m2), to obese (30 kg/m2 or higher).
Complication risks affected at different BMI cutoffs
Several types of complications increased at distinct levels of BMI, especially in the obese range. The risk of any complication increased at a BMI of 30 kg/m2 or higher. More severe obesity – BMI 35 kg/m2 or higher – was associated with increased rates of unplanned repeat surgery, including wound breakdown requiring reoperation.
Risk of infection requiring oral antibiotics increased at BMI 25 kg/m2 or higher, while infections requiring intravenous antibiotics increased at BMI 30 kg/m2 or higher. Higher BMI levels were also associated with increased rates of complications related to the abdominal donor flap, including infection and wound-healing problems.
Further analyses suggested optimal BMI cutoff point of 32.7 kg/m2 to minimize the occurrence of any breast complication and 30.0 kg/m2 for any abdominal complication. With a BMI of 32.7 kg/m2, the risk of breast complications was similar to that associated with current smoking.
The study demonstrates “a robust trend” whereby higher BMI levels are associated with increased complication rates for women undergoing autologous breast reconstruction. The findings suggest that targeting specific levels of weight loss before surgery might help to avoid postoperative complications.
“By quantifying the change in risk profile associated with a given change in BMI, our results can be used clinically to set evidence-based preoperative weight-loss goals for patients,” Dr. Piper and coauthors conclude. They emphasize that further studies would be needed to specifically evaluate the effects of weight loss before surgery.
Source:
Journal reference:
Barnes, L., et al. (2024) Relationship between Body Mass Index and Outcomes in Microvascular Abdominally Based Autologous Breast Reconstruction. Plastic and Reconstructive Surgery. doi.org/10.1097/PRS.0000000000010621.
An oral weight loss drug could help people with obesity who dislike needles
Kseniya Ovchinnikova/Getty Images
An experimental pill looks set to cause more weight loss than existing injectable treatments such as Ozempic, Wegovy and Mounjaro, based on early trial results reported on 7 March.
The medicine, called amycretin, caused people to lose 13 per cent of their weight over three months, more than twice the amount seen with Ozempic and Wegovy specifically. “This approach seems to be a little bit more exciting, from the limited data that we have,” says Daniel Drucker at the University of Toronto in Canada.
The results are from a placebo-controlled trial lasting three months, so it is too soon to know how amycretin stacks up against the other medicines for long-term effectiveness and safety, says Drucker, who wasn’t involved in the trial but has consulted for the manufacturer Novo Nordisk, as well as other pharmaceutical firms.
The diabetes drug Ozempic and the weight loss drug Wegovy are two brand names for the compound semaglutide. They work by mimicking a gut hormone called GLP-1 that is normally released after eating. This makes people feel full, reduces their appetite and boosts the release of the blood-sugar-regulating hormone insulin.
Semaglutide leads to the loss of about 15 per cent of body weight after it has been taken for one year, although weight then plateaus and people need to continue the injections long term or it tends to creep back up.
Another weight loss injection was launched last year, called Mounjaro, also known as tirzepatide or Zepbound. This mimics GLP-1 and an additional gut hormone called GIP. Mounjaro seems to lead to people losing about 21 per cent of their weight over the first year and five months of use, before their weight loss plateaus.
Amycretin, however, mimics GLP-1 and a different hormone called amylin, which seems to make it more potent still – at least over the first three months of treatment. People taking amycretin lost 13 per cent of their weight in this period, Novo Nordisk announced today, according to a report by Reuters. Those taking placebo pills lost 1 per cent. This is more than the equivalent figures for Wegovy and Ozempic, of 6 per cent, and for Mounjaro, of about 7.5 per cent.
However, we can only know for sure how the drugs measure up long term when they are compared under exactly the same circumstances in a single study, says Drucker. “These are not head-to-head trials.”
Another caveat is that medicines that work by mimicking GLP-1 have been used for more than a decade to treat type 2 diabetes and so their safety profile is well understood, which isn’t the case for an amylin mimic.
Novo Nordisk has also said that amycretin’s side effects were similar to those of Wegovy, which tend to be nausea, vomiting and diarrhoea, especially for people who increase the dose too quickly.
Being available in tablet form would be a great advantage for people who don’t like injections, says Daniel Chancellor at global pharmaceutical business analysts Citeline. “An oral pill is very attractive.”
As well as these three medicines, other weight loss drugs that mimic other gut hormones are also in development.
New findings reveal that the body undergoes significant, systematic changes across multiple organs during prolonged periods of fasting. The results demonstrate evidence of health benefits beyond weight loss, but also show that any potentially health-altering changes appear to occur only after three days without food.
The study, published today in Nature Metabolism, advances our understanding of what’s happening across the body after prolonged periods without food.
By identifying the potential health benefits from fasting and their underlying molecular basis, researchers from Queen Mary University of London’s Precision Healthcare University Research Institute (PHURI) and the Norwegian School of Sports Sciences provide a road map for future research that could lead to therapeutic interventions – including for people that may benefit from fasting but cannot undergo prolonged fasting or fasting-mimicking, such as ketogenic, diets.
Over millennia, humans have developed the ability to survive without food for prolonged periods of time. Fasting is practiced by millions of people throughout the world for different medical and cultural purposes, including health benefits and weight loss. Since ancient times, it has been used to treat diseases such as epilepsy and rheumatoid arthritis.
During fasting, the body changes its source and type of energy, switching from consumed calories to using its own fat stores. However, beyond this change in fuel sources, little is known about how the body responds to prolonged periods without food and any health impacts – beneficial or adverse – this may have. New techniques allowing researchers to measure thousands of proteins circulating in our blood provide the opportunity to systematically study molecular adaptions to fasting in humans in great detail.
Researchers followed 12 healthy volunteers taking part in a seven-day water-only fast. The volunteers were monitored closely on a daily basis to record changes in the levels of around 3,000 proteins in their blood before, during, and after the fast. By identifying which proteins are involved in the body’s response, the researchers could then predict potential health outcomes of prolonged fasting by integrating genetic information from large-scale studies.
As expected, the researchers observed the body switching energy sources – from glucose to fat stored in the body – within the first two or three days of fasting. The volunteers lost an average of 5.7 kg of both fat mass and lean mass. After three days of eating after fasting, the weight stayed off – the loss of lean was almost completely reversed, but the fat mass stayed off.
For the first time, the researchers observed the body undergoing distinct changes in protein levels after about three days of fasting – indicating a whole-body response to complete calorie restriction. Overall, one in three of the proteins measured changed significantly during fasting across all major organs. These changes were consistent across the volunteers, but there were signatures distinctive to fasting that went beyond weight loss, such as changes in proteins that make up the supportive structure for neurons in the brain.
For the first time, we’re able to see what’s happening on a molecular level across the body when we fast. Fasting, when done safely, is an effective weight loss intervention. Popular diets that incorporate fasting – such as intermittent fasting – claim to have health benefits beyond weight loss. Our results provide evidence for the health benefits of fasting beyond weight loss, but these were only visible after three days of total caloric restriction – later than we previously thought.”
Claudia Langenberg, Director of Queen Mary’s Precision Health University Research Institute (PHURI)
Maik Pietzner, Health Data Chair of PHURI and co-lead of the Computational Medicine Group at Berlin Institute of Health at Charité, said:
“Our findings have provided a basis for some age-old knowledge as to why fasting is used for certain conditions. While fasting may be beneficial for treating some conditions, often times, fasting won’t be an option to patients suffering from ill health. We hope that these findings can provide information about why fasting is beneficial in certain cases, which can then be used to develop treatments that patients are able to do.”
Pietzner, M., et al. (2024). Systemic proteome adaptions to 7-day complete caloric restriction in humans. Nature Metabolism. doi.org/10.1038/s42255-024-01008-9.
The Keto diet may be able to help people avoid weight gain
Shutterstock / Brent Hofacker
People with type 2 diabetes who stop using weight-loss drugs like Ozempic or Wegovy can avoid regaining the lost pounds if they adopt the ketogenic diet. The finding, which comes from a small study, challenges the notion that people must take these medications indefinitely to prevent unwanted weight gain.
Ozempic and Wegovy belong to a class of medications called GLP-1 agonists, which reduce appetite and boost the release of insulin. They are commonly prescribed to help people with type 2 diabetes regulate blood sugar and lose weight. However, the assumption has been that people must remain on the drugs long-term otherwise they regain the lost weight.
Shaminie Athinarayanan at Virta Health – a US telehealth company that treats type 2 diabetes – and her colleagues decided to test that assumption. Their inspiration for doing so came from previous research showing that low-carbohydrate diets, like the ketogenic diet, help manage blood sugar levels and weight in people with type 2 diabetes.
The researchers tracked weight and blood sugar levels in 308 adults living in the US with type 2 diabetes who received nutrition therapy at Virta Health. All of them were using GLP-1 agonists when they enrolled. Participants were advised to follow the ketogenic diet – meaning they were told to eat less than 30 grams of carbohydrates daily, or less than 50 grams if they were vegan, and about 1.5 grams of protein per kilogram of bodyweight. They were encouraged to eat until they felt full, regardless of calories. Health coaches and licensed medical professionals virtually communicated with participants as needed.
Between three and nine months later, half of the participants discontinued using GLP-1 agonists. All participants continued to follow the ketogenic diet for an additional year. At this point, the researchers found there were no significant differences in weight or blood sugar levels between the two groups. On average, participants who stopped taking GLP-1 agonists only gained about a kilogram of weight. By comparison, those who continued taking the medications gained about two kilograms. Most of the participants in both groups also had blood sugar levels below the threshold for diagnosing diabetes.
“This study suggests that the continued use of GLP-1 agonists is not necessary for many people if [they] have the right intervention,” says Athinarayanan. “You can discontinue [these medications] safely and effectively and maintain weight and blood sugar outcomes.”
This may be helpful for people who can’t take these medications due to shortages or side effects, says Priya Jaisinghani at NYU Langone Health. However, people must speak with their doctor before beginning a low-carb diet since it can carry risks, especially for those with underlying conditions like kidney disease or an eating disorder, she says. She also points out that the study was sponsored by Virta Health and only included a small number of participants. So, “It is not the end all be all”, says Jaisinghani. “But it shows the difference diet can make.”
Pharmaceutical companies that manufacture insulin made headlines last year when they voluntarily agreed to provide discount cards that lower the monthly cost of insulin for many people to $35.
But getting your hands on this card — and persuading a pharmacist to accept it — can be a hassle.
In this episode of “An Arm and a Leg,” producer Emily Pisacreta speaks with “insulin activists” and pharmaceutical experts to find out what this change in prices means for people with diabetes and why the fight for affordable insulin isn’t over yet.
Host and producer of “An Arm and a Leg.” Previously, Dan was a staff reporter for Marketplace and Chicago’s WBEZ. His work also appears on All Things Considered, Marketplace, the BBC, 99 Percent Invisible, and Reveal, from the Center for Investigative Reporting.
Note: “An Arm and a Leg” uses speech-recognition software to generate transcripts, which may contain errors. Please use the transcript as a tool but check the corresponding audio before quoting the podcast.
Dan: Hey there. Right after the holidays, I got an email from a listener named Brianna.It started, “Happy new year Dan! I was just reading the news about the price of insulin going down to $35! Is that for everyone?”
And I was like, Huh. I had a sense that there was some news about the price of insulin, but 35 dollars a month for everyone? That sounded like a BIG reduction. And big news.I googled the latest stories, and I was… not totally sure what I was seeing.
I was definitely seeing some new stories about people paying 35 bucks from here on out. And there seemed to be some federal law involved, and politicians were patting themselves on the back. But it just wasn’t totally clear: Was insulin now 35 dollars for everyone? Did the outrageous price of insulin get solved while I wasn’t looking?
And I mean, I’ve kinda been looking. We’ve done a couple of episodes about the price of insulin already — because insulin is iconic. It represents the wild cost of prescription drugs in this country. More than 8 million Americans take insulin to treat their diabetes – and for some, going without it could actually kill you.
And its price got jacked up so much — huge multiples over like ten years — — that one in four of those people who couldn’t go without… took to rationing: Seeing how much they could go without, short of actually dying.
So I asked our senior producer Emily Pisacreta to take the case.
Emily: I feel more like the senior insulin correspondent, which is fine with me as the resident type 1 diabetic! And a lot has happened since the last time we talked about insulin on this show. We really do need an update.
Dan: This is an “Arm and a Leg”, a show about why healthcare costs so freaking much, and what we can maybe do about it. I’m Dan Weissmann, I’m a reporter and I like a challenge. So our job here is to take one of the most enraging, terrifying, depressing parts of American life, and bring you something entertaining, empowering and useful.
Today we have a question: what’s going on with insulin? Is it $35 now?
Emily: Well, there have been some BIG improvements — bigger than I thought when I started reporting. A lot of people can get their monthly supply of insulin for just $35. But it is oversimplified to say it just costs $35 now. And the people who have been fighting to lower the price of insulin over the past decade? They’re still very pissed. So let me walk you through what changed, what led to those changes, and what’s still unresolved.
Dan: OK!
Emily: For years now, there’s been a giant push from people with diabetes to get the federal government to do something about the high cost of insulin. In 2022, finally something came through. I’m talking about a provision in Inflation Reduction Act.
Dan: Yes– I remember this– the Inflation Reduction Act was a big infrastructure bill that included, like renewable energy subsidies, and– honestly, this is the reason that I remember the bill, because we did an episode about this part– letting medicare negotiate some drug prices?
Emily: Exactly. It said people on Medicare would be able to get a month’s supply of insulin for no more than $35 out of pocket. But of course that left a big gaping hole. BECAUSE that’s cool for people on Medicare, but what about the rest of us? And the pharma companies were feeling the heat. Here’s President Biden in his State of the Union last year:
President Biden: Big pharma has been unfairly charging people hundreds of dollars, four to $500 a month making record profits. Not anymore. Not anymore.
Emily: By the way, those pharma companies? There’s three of them who make insulin.
That’s the American company Eli Lilly, the Danish company Novo Nordisk, and the French company Sanofi. OK so: not long after Joe Biden talked about their record profits, the insulin makers were back in the news. …
Eli Lilly was the first to announce they were going to slash prices on several of their most popular insulins, and limit out of pocket spending to $35 a month.
Fox News: This is a big story.
Next, Novo Nordisk and Sanofi made similar announcements.
CNN: Millions of Americans are affected by this major news this morning for millions of people suffering from diabetes and high prescription drug costs.
Basically, the insulin manufacturers all said hey, you’re not covered by this Medicare thing? We’re going to bring your copay down to $35 ourselves. So if you have commercial insurance Print out this card, take it to the pharmacy, and your copay will be no more than $35 for a month’s supply of insulin.
Dan: And what if you’re uninsured?
Emily: Well, they have a card for that, too.
Dan: OK so what I’m hearing is you need a card.
DAN: Yes. How do you get one?
Emily: The insulin makers set special phone numbers you can call. Or you can visit their websites, fill out a little form, and download the card.
Dan: Sounds simple, unless I’m missing something?
Emily: In all honesty, I had no problem with those steps. But I wouldn’t assume that’s the case for everyone. And I’m also not rationing insulin right now.
Zoe Witt: When you are rationing insulin, maybe you aren’t even fully rationing insulin yet, but you don’t know how you’re going to get Your next prescription, your next fill of insulin…You are in crisis. Like, you, you do not have the capability to sift through these websites. It’s very confusing. It’s very overwhelming.
Emily: This is someone who frequently speaks to people struggling to afford insulin.
Zoe Witt: my name is Zoe Witt. I work with Mutual Aid Diabetes.
Emily: Mutual Aid Diabetes. That’s an all volunteer group that has banded together to help diabetics get what they need, when they need it. They help people with cash and with free diabetes supplies, including insulin, no questions asked. That means Zoe knows the ins and outs of every obstacle to getting insulin.
Zoe Witt: Our healthcare system is like a whack a mole from hell.
Emily: And Zoe reminds me: if you’re not taking enough insulin, you probably feel awful. Maybe not even thinking straight. And it can affect your eyes, making it hard to read.
Zoe Witt: It just is unmanageable
Emily: Zoe says they talk with people all the time who are too stressed out or too debilitated to download these cards and use them. Diabetes folks walk people through the process. And once someone has the card… Mutual Aid Diabetes gives people the 35 bucks, too, if they say they need it. Because $35 can be a barrier for a lot of people. And it’s actually $70 sometimes if you use 2 types of insulin at once, which lots of people do… myself included.
Dan: Wow. OK. But then once people have the cards they typically have no problem?
Emily: Well, your pharmacist has to know what they’re doing, too. So sometimes it means a patient having to educate their pharmacist– or even bring the doctor in to help troubleshoot — which is no picnic. And people with diabetes are always having to deal with insurance roadblocks at the pharmacy, so I don’t want to make anything sound simpler than it is.
Dan: It’s like a whack a mole from hell!
Emily: Exactly! And the cards don’t solve everything. Especially this: if you have insurance, these cards only apply to the insulin your insurance plan already covers. If you normally need a prior authorization to get the right insulin for you… that is still the case.
Dan: Right. Okay. like prior authorization is this roadblock to getting all kinds of treatment, that you and your doctor agree that you should have, and your insurance company can say, we disagree. We’re s not authorizing this. And then you’re stuck.
Emily: Right.
Dan:But in terms of what the pharma companies. can do to kind of offer you a deal. They’re basically doing it. Is that right?
Emily: I think that’s fair to say.
Dan: That’s super interesting. All right. So it’s not solved, but this is a big step forward. And what’s not solved is: some people are still on the hook for the list price for insulin — the price without any discounts or insurance or whatever. But you found big improvements there too, right?
Emily: Yes! When the companies announced all these discount cards, they announced a whole other big change, too. Slashing the list prices of a bunch of different insulins by up 75%. So a vial that once was north of $300 is now being listed at around $70.
Dan: OK, that sounds like a big improvement.
Emily: It’s a big, big deal. Actual price reductions are what diabetes advocates have been demanding all along. And… while these are still the highest prices in the world for these same insulins, to see them drop from triple to double digits, it’s wild.
Dan: I sense that there’s a “but” here.
Emily: Well, the Big Three didn’t lower the price of every type of insulin, only ones that have been around since the 1990s or early 2000s. Newer insulins that work faster or last longer are not included here.
Dan: And I’m guessing not all insulins work the same way.
Emily: Right. Some people can switch between types or brands of insulin easily. For other people, there can be allergies or one works better with their body with another kind. It’s complicated. It’s medicine! AND… there have been some issues with pharmacies actually stocking lower list price insulin. That is a whole ‘nother saga… an episode for another day. But the important thing is… a bunch of insulin is a lot cheaper now.
Dan: Wow. Emily, you said right at the top: The changes here are bigger and better than you realized before you started reporting.
Emily: Yes but there’s still a lot more to say.
Right. After the break, we’ll’ hear from you about why these changes happened NOW. And what it means for people with diabetes and really all of us…
[midroll]
So. We have seen some big changes in the last year — including DRUG COMPANIES expanding their discount programs and lowering the sticker prices on insulin, dramatically. Why now? I’m guessing this wasn’t because they had a big change of heart.
Emily: I can’t speak to what’s in pharma’s hearts. But I did talk to someone who knows a lot about pharma’s brain.
Ed Silverman: my name is Ed Silverman, and I work at Stat News, a health and life sciences website,
Emily: I’m a big fan of Stat News
Dan: Me too, man! Their reporting is great.
Emily: And Ed Silverman. He’s been covering the pharmaceutical industry for almost 30 years. He thinks activism from people with diabetes over the years created political pressure that played a big role in the decision to slash prices. But there was also something kind of hidden at work.
Ed Silverman: It’s not altruism, here was a real mechanism, government mechanism in place that helped change the equation and therefore the thinking back at the companies.
Dan: OK… what is he talking about?
Emily: So, Dan: do you remember the stimulus bill, the American Rescue Plan?
Dan: I’m starting to feel like this episode is a quiz on recent-ish legislation. And I think I’m gonna do pretty well here:.The American Rescue Plan was a trillion dollar stimulus that Joe Biden got passed right after he got into office– am I right?
Emily: OK, hotshot. Do you remember how in part 8 section 9816 they sunsetted the limit on the maximum rebate for single source drugs and innovator multiple source drugs?
Dan: Um, busted. No.
Emily: Ok so here’s the deal: it’s obviously kinda wonky so I’ll simplify– in that little section Congress made a tweak to Medicaid, basically raising penalties on drug-makers for jacking up prices too far, too fast. So if you’re a pharma company who has raised the price of a drug by a lot very quickly, which is true of insulin, and a lot of people on Medicaid use your drug, which is also true of insulin, then you have to pay a big penalty. In the case of insulin, that penalty would be more than you’d make selling the insulin to Medicaid. A LOT more: So, unless you bring the price back down, you’re going to owe Medicaid a lot of moolah. And those penalties were set to kick in January 1st 2024.
Dan: So you’re telling me: Part of what the pharma companies did here came right out of a small part of a giant federal law from 2021.
Emily: Yep. And there’s another big wheel turning in the background here. Novo Nordisk and Eli Lilly, two companies who really got their start by selling insulin, now make other diabetes drugs — drugs that are now increasingly used for weight loss. And it’s a bonanza.
GMA: It is literally the hottest drug in the country right now.
Fox News: all people are talking about these days is Ozempic, wegovy. Oh my gosh, this person lost 20 pounds. This person lost 50 pounds.
Ozempic Ad: [Jingle:] “Oh, Oh, Oh, Ozempic!
[Announcer:] Once weekly Ozempic is helping many people with type 2 diabetes like James lower their blood sugar.
Emily: Drugs like Ozempic, Wegovy, Mounjaro. They’ve been in super high demand. And there’s been a ton of hype about their various potential health benefits. For weight loss, for heart health. Scientists are even interested in whether it can help people with substance use disorders. Meanwhile, for Eli Lilly and Novo Nordisk, the returns on these drugs dwarf anything else they’re selling. Novo Nordisk even became the biggest company in Europe – for like a minute… but still.
Dan: OK, this is interesting, but what does it have to do with the price of insulin?
Emily: I’d wondered… maybe these companies can just better afford to buy some political peace by lowering insulin prices, because they are making so much bank on these new drugs, ? Ed Silverman had a take on that.
Ed Silverman: It makes perfect sense that these cash cows, these medicines that are used for diabetes and, weight loss are going to become increasingly important to their bottom line more than other medicines
Emily: More than insulin. And they’re selling so much so fast, they can hardly keep up with demand. Which could end up affecting people who need insulin.
Dan: Wait, how?
Emily: Look, for example, in November, Novo Nordisk said they were investing 3 and half billion dollars into ramping up production of injection pens for Wegovy, one of their top drugs in this category. Less than a week later, Novo announced they would be phasing out one of their insulin products from the US market – an insulin called Levemir. It’s one of the insulins whose prices they just dropped. And… coincidence… Levemir also comes in a pen.
Dan: So Novo Nordisk is phasing out an insulin pen so they can make more Wegovy pens?
Emily: Well, we don’t know that for sure. But Novo Nordisk did tell me that “manufacturing constraints” were part of why they’re dumping Levimir. They said it was one of several reasons and also wrote: “We made this decision after careful consideration and are confident that given the advanced notice, U.S. patients will have access to alternative treatments and can transition to other options.
Dan: Huh. OK.
Emily: But even if pulling this insulin Levemir off the market had nothing to do with their trouble meeting the demand for their big blockbuster drug… it brings to mind an important question about all the changes we talked about today — whether it’s the copay savings or the lowered list prices. Here’s Ed Silverman.
Ed Silverman there’s no guarantee that the companies will keep these in place. Maybe after time, some of the attention on insulin is diverted and maybe eighteen months from now, one company might quietly roll back some of the Benefits, if you want to use that word, there’s nothing requiring them to maintain the steps they’ve taken.
Emily: I asked all three insulin makers about this. None of them promised there would never be any backsies. Lilly wrote back “Lilly is committed to ensuring all patients can access any Lilly medicine they need” — and touted their efforts to date. Similarly, Sanofi wrote “We continually review our affordability offerings to support our aim that no one should struggle to pay for their insulin. Novo Nordisk’s response was “Novo Nordisk increases the price of some of our medicines each year, in response to changes in the healthcare system, market conditions, and the impact of inflation.”
Dan: Yeah, that especially does not sound like a pinky-swear, no-backsies kind of response.
Emily: AND that’s not much comfort for insulin activists. Folks like Shaina Kasper, who works for T1International. They’re a group that’s been at the forefront of this fight for years. I Asked her…
Emily-on-tape: So is this issue of high insulin prices just resolved now?
Shaina Kasper: No, it hasn’t been. It’s been really frustrating…
Emily Shaina and others are worried that the announcements from the manufacturers about savings cards and voluntary list price reductions will take the pressure off the government to do something more sweeping. Because for now…
Shaina: The manufacturers really hold all of the power here And if patients are counting on these programs to literally be able to survive, that has life and death consequences
Dan: This question about who holds the power, it reminds me of a story we did a few months ago… the one about how the writer John Green led a kind of online crusade targeting the drug-maker Johnson & Johnson. And how, even though the pressure campaign worked — J & J ended up allowing lower-priced versions of an important tuberculosis drug — activists who worked on the issue were like: It’s a problem that Johnson & Johnson has the power to say yes or no here..
Emily: Exactly. That which pharma giveth, pharma can taketh. At least the way things are set up now. Now I should say, all three companies told me they plan to continue their affordability offerings. But if insulin continues to be the poster child for high drug prices, prices virtually everyone in America agrees are too high…it does raise the question: are voluntary programs from pharmaceutical companies the solution we want? To Zoe from Mutual Aid Diabetes, the answer is no. They find these manufacturer savings cards kind of a bitter pill… no pun intended.
Zoe Witt: there’s certainly no justice in these programs,
Emily: And zoe for one would say that justice is overdue.
Zoe Witt: These companies have price gouged us. for years, making obscene amounts of money. Then, presumably, as, we’re often told is the justification for these ridiculous prices, they did research and development for more diabetes drugs, which are Ozempic, Monjoro, etc. And now, these companies, for, the next 15 years, are set to make, billions and billions of dollars, on these drugs,
Emily: I asked the big three insulin manufacturers about what Zoe said – about how angry folks like them are over the cost of insulin. Novo Nordisk said “we continually review and revise our offerings as well as work with diverse stakeholders to create solutions for differing patient needs. ” And Sanofi and Lily both said something very similar.
Emily: So… in the end– or at least for now– here’s the answer to our listener’s question…. There are more avenues than ever to get a month’s supply of insulin for $35. Great. It may be a lot easier to avoid rationing your insulin now than it was a couple years ago. That’s also really great. But people with diabetes do not think this fight is over.
Dan: So what DO they want?
Emily: Some people still want the federal government to just put a cap on what people pay for insulin, like by law.. Others are working to build alternatives to the existing pharmaceutical industry, like California’s CalRx program.
Dan: Cal Rx… now you’re calling back our story from the last time we talked about insulin.
Emily: Yep, Cal Rx is the state of California’s attempt to enter the insulin market, to introduce some low priced generics and sell them essentially at cost. Other states are joining in. Even if some of these specific plans fall apart — even if California somehow can’t get its government-sponsored insulin to market, even if Pharma rolls back some of the discounts…the past few years have been enormous for people with diabetes. Mostly because they’ve found each other.
Zoe Witt: I was rationing insulin in 2018, I didn’t even know that there was a term for it. I didn’t know other people were doing it. I know a lot of people died that year. And there were multiple occasions where I, in retrospect, definitely almost died. And the one good thing that has, that has happened between now and then is that people have been talking about it and People are now more comfortable telling others that they’re struggling, that they can’t get their insulin.
Emily: Connecting with Mutual Aid Diabetes or other networks to get or give help.
Zoe Witt: We’re all keeping each other alive, like to me, that’s the number one thing that has changed.
Emily: I think that’s a huge lesson here, and a takeaway that’s not new on this show. Keeping each other alive — or even just keeping each other from getting bankrupted by the medical system — is up to us. And while a mutual aid group modeled exactly like Mutual Aid Diabetes may not work for every disease or every drug, Zoe says they’re more than willing to talk to anyone who might be interested in trying.
Zoe Witt: I mean, we’ve even had people ask, like, is there like a mutual aid asthma or something like for inhalers?
Emily: Their advice?
Zoe Witt: I think that, you know, to start, you would want, like, probably at least, like, five to ten “ride-or dies,” like, people that are really willing to, like, go the extra mile,
Dan: Five to ten– that just does not sound like that many! (I mean, I think.) One thing I’m taking away is: This is a lot of activism over a long time, that eventually had a big effect. Another thing I’m taking away here? Sneaky policy changes — like lifting the Medicaid rebate cap — can make a huge difference. God bless whatever nerds are writing the next little bit of law to sneak into a giant bill, like a hacker with a virus.
Emily: Totally. OK. I gotta take a shot, and eat my lunch.
Dan: Go for it. We’ll be back with a new episode in a few weeks. Till then, take care of yourself.
This episode of an arm and a leg was produced by Emily Pisacreta and me, Dan Weissman and edited by Ellen Weiss.
Adam Raymonda is our audio wizard. Our music is by Dave Weiner and blue dot sessions.
Gabrielle Healy is our managing editor for audience. She edits the first aid kit newsletter.
Bea Bosco is our consulting director of operations. Sarah Ballama is our operations manager.
And Arm and a Leg is produced in partnership with KFF Health News. That’s a national newsroom producing in depth journalism about healthcare in America and a core program at KFF, an independent source of health policy research, polling and journalism.
Zach Dyer is senior audio producer at KFF Health News. He’s editorial liaison to this show.
And thanks to the Institute for Nonprofit News for serving as our fiscal sponsor, allowing us to accept tax exempt donations. You can learn more about INN at INN. org.
Finally, thanks to everybody who supports this show financially– you can join in any time at arm and a leg show dot com, slash, support — and thanks for listening.
“An Arm and a Leg” is a co-production of KFF Health News and Public Road Productions.
In a recent study published in the journal Nature Metabolism, a team of scientists investigated whether modulation of the gut microbiome using dietary fiber supplementation in the form of resistant starch could help with insulin resistance and weight loss and offer a potential treatment avenue for metabolic disorders.
Obesity has been classified as a global epidemic, with substantial research being conducted on strategies to reduce weight and prevent obesity. It contributes significantly to the global mortality rates by increasing the risk of metabolic diseases such as diabetes, as well as cardiovascular disease risk. Weight management and effective weight loss can lower the risk of these diseases.
Increasing evidence indicates that the gut microbiome plays a pivotal role in the regulation of human physiology and development of various diseases. Gut microbiome composition and diversity are intricately linked to the metabolism of glucose and fat and inflammation.
Furthermore, while fecal microbiome transplantation has been used to establish healthy gut microbiome communities, the procedure has not yielded effective or long-term results. However, diet can be used to modulate the gut microbiome, and dietary interventions, either alone or in conjunction with fecal microbiome transplantation, could potentially improve the clinical outcomes.
About the study
In the present study, the team conducted a randomized, crossover clinical trial involving overweight individuals to determine whether dietary supplementation with resistant starch positively impacted obesity and metabolic phenotypes. They also conducted metagenomic and metabolomic analyses to understand how the resistant starch affected the composition of the gut microbiome and its function.
Furthermore, they studied antibiotic-treated mice that had received gut microbiomes from human donors that had already been modified through resistant starch supplementation to understand how gut microbiomes modified through supplementation with resistant starch influence glucose metabolism and adiposity. The metabolomic advantages offered by the gut microbiome modified through resistant starch supplements were also explored.
Resistant starch cannot be broken down by the amylase enzymes produced in humans, functioning as a dietary fiber. During digestion, resistant starch does not get broken down in the stomach or small intestine but moves into the large intestine or colon, where the gut microbiome ferments this dietary fiber. Rodent model studies have shown a decrease in body fat and better metabolic outcomes when the carbohydrate portion of their diet consists mainly of resistant starch.
The present clinical trial included participants with excess body weight who did not have any chronic disorders, were not using any probiotics or antibiotics, and were not undergoing any treatments that would impact their glucose metabolism. The participants were randomly assigned to the treatment or control group, with the treatment group receiving resistant starch in the form of high-amylose maize and the control group receiving amylopectin with no resistant starch.
The starch was provided in sachets in powdered form, and all the participants in the treatment and control groups consumed one packet of the appropriate starch twice a day before a balanced, isoenergetic meal that was provided thrice a day. Since this was a crossover clinical trial, all the participants underwent two eight-week-long interventions, one for the resistant starch treatment and the other for the control treatment.
Results
The results showed that supplementation with resistant starch helped achieve a mean weight loss of about 2.8 kg and improved insulin resistance in overweight participants. The study also found that the beneficial effects of resistant starch supplementation were associated largely with gut microbiome composition changes.
The bacterium Bifidobacterium adolescentis was found to be associated with resistant starch supplementation in humans, and the monocolonization of mice with this bacterium protected them from diet-induced obesity. Resistance starch impacted lipid and fat metabolism by reducing inflammation, restoring the intestinal barrier, and altering the bile acid profile.
The gut microbiota impacts the host physiology through signaling metabolites, of which bile acids play a significant role. Secondary bile acids, such as glycodesoxycholic acid, deoxycholic acid, glycocholic acid, and taurodeoxycholic acid, are important in improving insulin sensitivity and ameliorating hepatic steatosis. The enzyme bile salt hydrolase carries out the deconjugation of secondary bile acids.
The study found that resistant starch supplementation decreased the production of bile salt hydrolase and increased the levels of secondary bile acids. The results were reciprocated in the mice after they were monocolonized with B. adolescentis from humans who underwent resistant starch supplementation.
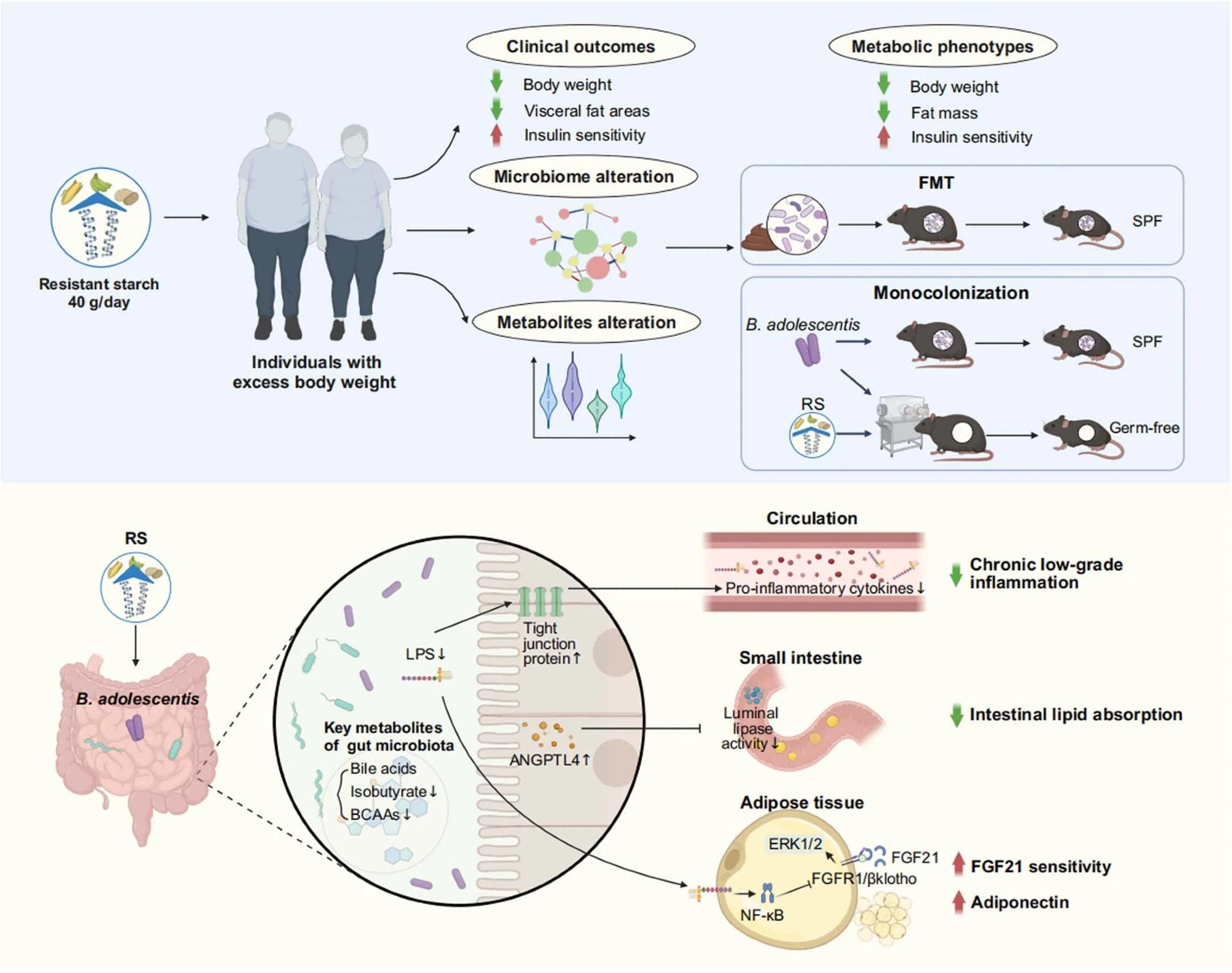
Resistant starch (RS, 40 g d-1) accompanied with isoenergetic and balanced diets led to an obvious reduction in body weight and improvement of insulin sensitivity, as well as alteration in metagenomics and metabolomics. Faecal microbiota transplantation (FMT) showed benefits of RS were associated with the reshaped gut microbiota composition. Monocolonization of mice with B. adolescentis, which was closely correlated with the benefits of RS in human protected mice from diet-induced obesity. Mechanistically, the RS-induced changes in the gut microbiota influenced metabolites of gut microbiome, reduced chronic low-grade inflammation by improving intestinal integrity, inhibited lipid absorption by modulating angiopoietin-like 4 (ANGPTL4), and improved the sensitivity of fibroblast growth factor 21 (FGF21) in adipose tissue. SPF, specific-pathogen-free; LPS, lipopolysaccharide; BCAAs, branched-chain amino acids; Erk1/2, extracellular signal-regulated kinase 1/2; FGFR1, fibroblast growth factor receptor 1. Created with BioRender.com.
Conclusions
To summarize, the study found that supplementation with resistant starch can facilitate weight loss by increasing the abundance of B. adolescentis in the gut microbiome. It can also help improve insulin sensitivity through gut microbiome-induced changes in the levels of secondary bile acids and lowering of inflammation.
Journal reference:
Li, H., Zhang, L., Li, J., Wu, Q., Qian, L., He, J., Ni, Y., KovatchevaDatchary, P., Yuan, R., Liu, S., Shen, L., Zhang, M., Sheng, B., Li, P., Kang, K., Wu, L., Fang, Q., Long, X., Wang, X., & Li, Y. (2024). Resistant starch intake facilitates weight loss in humans by reshaping the gut microbiota. Nature Metabolism. DOI: 10.1038/s4225502400988y, https://www.nature.com/articles/s42255-024-00988-y
A supplement containing a kind of carbohydrate that takes longer to be digested, called resistant starch, has helped people lose a modest amount of weight in a small trial.
Resistant starch is naturally found in beans, wholegrains, raw oats and green bananas, and also forms when common starchy foods like potatoes, pasta and rice are left to cool down after being cooked.
There are several different forms of resistant starch, but what they have in common is that the structure of the molecules means they can’t be easily digested and absorbed in the small intestine.
The starch therefore reaches the large intestine, further along the gut, where it is digested by bacteria, meaning it is classed as a prebiotic.
While some previous studies have suggested that this starch can help people lose weight, Huating Li at Shanghai Jiao Tong University School of Medicine in China and her colleagues investigated its effects on our gut bacteria.
They asked 37 overweight people to consume a sachet of starch mixed with water twice a day before meals. For eight weeks, they were given resistant starch, while, for another eight weeks, the packet contained ordinary starch as a comparison. Participants were also provided with three balanced meals a day and various health indicators were measured.
After having the resistant starch for eight weeks, people lost an average of 2.8 kilograms, while the ordinary starch had no effect on weight. The resistant starch also caused less of a rise in blood sugar after meals, which may be good for health.
Stool samples revealed that while people were taking resistant starch, several bacterial species became more numerous in their guts. When these bacteria were transplanted into mice that were given a high-fat diet, they seemed to have a weight-reducing effect.
Rebecca McManamon, a spokesperson for the British Dietetic Association, says the trial was too small to be definitive, but the findings are plausible. “It’s logical that these results would happen,” she says.
However, some people with irritable bowel syndrome may find that eating resistant starch results in bloating and discomfort due to the bacteria creating gas as they break it down, she says.